-
18 July 2025 | Country Update
France expands smoking ban in outdoor public areas -
21 October 2024 | Country Update
Reimbursement of new prevention consultations provided by physicians, nurses, midwives, and pharmacists
5.1. Public health
5.1.1. Principal public health institutions and authorities
The French Public Health Agency (Santé publique France, SPF) is the principal agency responsible for public health policy and expertise in France. Its missions, defined in the Public Health Code (Public Health Code of 1 May 2016), include health promotion and education, public health surveillance, and disease prevention and monitoring, as well as alert and response to disease outbreaks and other public health emergencies. The agency was created in the 2016 Health Reform Law (Law no. 2016-41 of 26 January 2016) under the umbrella of the MoH. The SPF regrouped four former public agencies: the National Institute for Health Monitoring (Institut de veille sanitaire, InVS), the National Institute for Prevention and Health Education (Institut national de prévention et d’éducation pour la santé, INPES), the Agency for Health Emergency Response and Preparedness (Établissement de préparation et de réponse aux urgences sanitaires, EPRUS) and a non-profit drug and alcohol addiction prevention service (Addictions drogues alcool info service, ADALIS). The SPF relies on regional branches (Cellules d’intervention en région, Cire) located within the ARS to support them with scientific expertise on health monitoring, surveillance and alerts at the local level (ARS Pays de la Loire, 2021).
The ARS are in charge of coordinating all health-related agencies and care providers in their region (section 2.3). Their public health responsibilities include implementing national policies at the regional level, such as organizing and financing disease monitoring and surveillance, health promotion and disease prevention activities, and managing public health emergencies at the local level (ARS, 2014).
In France the MoH is responsible for public health policies, including prevention (such as the national vaccination programme) and health promotion (MoH, 2015a). The HAS, an independent scientific administrative authority, oversees the development of guidelines of good practice for medical care. The HAS is also in charge of providing guidance on national screening and prevention programmes. It has a Technical Commission on Vaccinations (Commission technique des vaccinations, CTV), which issues recommendations on vaccination strategy and schedule (HAS, 2017a).
The HCSP provides the government with expertise for developing and evaluating public health policies and for managing public health risks and safety (Public Health Code of 1 May 2016) (Milon et al., 2020).
Municipalities have a limited role in public health, apart from sanitary and environmental management (of water supply, waste disposal, food and industrial hygiene) for which they are responsible (Code of Local Authorities of 23 August 2021). However, municipalities can engage in health promotion and disease prevention on a voluntary basis – for instance through “local health contracts” signed with the ARS for implementing joint health promotion and disease prevention projects (ARS, 2012), or by participating in the World Health Organization Healthy Cities Network (WHO, 2021).
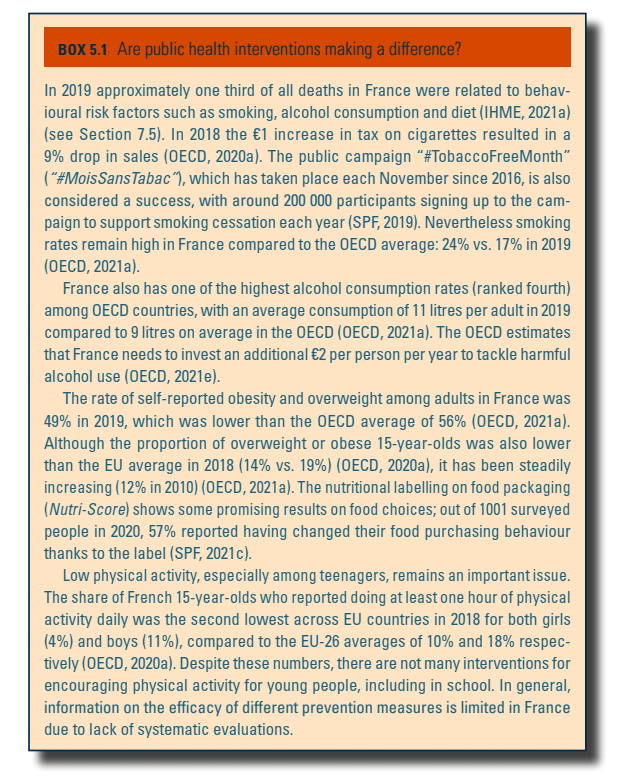
Box5.1 discusses the effectiveness of public health interventions.
Box5.1
5.1.2. Response to disease outbreaks
The National Prevention and Management Plan against influenza pandemics (SGDSN, 2011) is used as a guide for all infectious disease outbreaks. The plan has four stages adapted to the severity of the spread. The first stage consists of preventing the virus from entering the national territory through limiting international travel and quarantining individuals arriving from affected countries. Once the virus is in the national territory, the second stage seeks to limit the spread of the virus (for instance through limiting public gatherings and quarantine of infected individuals and their contacts). In the case of a national epidemic, the third stage aims to limit its effects (for instance through closing schools and reinforcing health personnel treating infected patients). The fourth and last stage consists of a recovery phase (for instance with financial aids to vulnerable populations and evaluations of the disease outbreak response) (SGDSN, 2011). Several agencies share the active response to a disease outbreak. The SPF manages the centralized monitoring and response to infectious diseases, while the HAS provides guidance and directives for health professionals on the treatment of patients. The medical products and clinical trials related to the epidemic are evaluated and approved by the ANSM.
During the Covid-19 pandemic the National Prevention and Management Plan was mobilized. The SPF oversaw the monitoring of the epidemic and published statistics on the spread of Covid-19, including the numbers of daily cases, hospitalizations and tests performed, etc. However, the SPF and its local branches were slow in developing a public health response, and in defining the prevention strategy. The SPF was criticized for being undersized in terms of skills and staff, and for being unprepared for a pandemic. The agency had difficulties in building up and managing strategic stocks (including protective materials), but also in developing a quick operational response to the health crisis (Borowczyk & Ciotti, 2020; Or & Gandré, 2021).
5.1.3. Immunization
The MoH is responsible for the national vaccine programme, which is issued and updated based on recommendations established by the HAS (MoH, 2021f).
Eleven vaccines are mandatory for children and free of charge in France: diphtheria, tetanus and polio since 1938, 1940 and 1964 respectively, and eight since 2018 (pertussis, Haemophilus influenzae type b, hepatitis B, pneumococcal infections, invasive meningococcal infections of serogroup C, measles, mumps and rubella) (MoH, 2021f ). Children who have not received these vaccines are not allowed in day care and schools (Service public, 2021). A twelfth vaccine – against yellow fever – is mandatory in the overseas territory of French Guyana.
In addition to the 11 mandatory vaccines, there are some recommended vaccines for specific population groups, of which the cost is partly (65%) covered by the SHI. This is for instance the case for vaccination against human papillomavirus, which is recommended for teenage girls and, since 2021, for boys. Complementary vaccination protocols exist for vulnerable populations and emergency vaccination responses, such as to Covid-19 (MoH, 2021f ).
Vaccination of the general population mainly relies on GPs and paediatricians. However, since 2022 nurses are allowed to inject a large number of vaccines to adults and children aged over 16 without a medical prescription (Decree no. 2022-610 of 21 April 2022) (previously they were limited to tuberculosis and influenza vaccines) (Public Health Code of 2021). Since 2022 pharmacists can also carry out such vaccinations upon a medical prescription (Order of 21 April 2022a). They have been able to vaccinate older people against seasonal influenza without a medical referral since 2019. Midwives have been allowed to vaccinate women and infants against specific diseases since 2016 (Order of 10 October 2016) and the list of vaccines they can administer was extended in 2022 (Order of 21 April 2022b). Maternal and child protection services (Protection maternelle et infantile, PMI) and occupational physicians can also deliver vaccinations (Public Health Code of 2022).
While vaccine coverage has increased over the last decades (SPF, 2020), in 2019 the percentage of children vaccinated against hepatitis B, pneumococcal and meningococcal infections, and measles was still below the WHO recommendation of 95% (MoH, 2021f ). France has a high prevalence of vaccine hesitancy; in 2016, 25% of the population had negative views towards vaccination in general and 41% had a negative opinion on at least one vaccine (SPF, 2017). Given this well known vaccine hesitancy, the government put significant effort in developing an efficient vaccination campaign against Covid-19 with emergency legislation allowing more professional groups to carry out vaccination (such as firefighters, dentists, veterinarians and physiotherapists) (Order of 7 July 2021). Large ad hoc vaccination centres, which recruited retired health professionals, nurses and students, were also set up (HSRM, 2021). Despite all these measures, vaccination rates were low in the first half of 2021, especially amongst the most deprived populations (Spire, Bajos & Silberzan, 2021). The government hence applied unprecedented restrictions and incentives to support the uptake of the Covid-19 vaccination. These measures included suspension, without remuneration, of unvaccinated professionals who were in close contact with the public (health and social care workers, firefighters, the army, etc.), and an obligation to show a Covid-19 certificate with proof of vaccination or antibodies against Covid-19 (or a negative Covid-19 test but this possibility was later suspended) for employees, customers and visitors in public and commercial places (such as restaurants, cinemas, museums, sports facilities and shopping malls) and in long-distance public transport (Law no. 2021-1040 of 5 August 2021). These measures significantly increased vaccination rates, with an estimated 72 151 additional doses per million inhabitants, or 4 874 857 additional doses in absolute terms 40 days after the announcement (Mills & Rüttenauer, 2022). Despite initial resistance, vaccination rates were also boosted for health professionals, especially in nursing homes, and the share of staff being suspended was estimated to be very low. The Covid-certificate was also used for encouraging a third booster dose in early 2022, but it is not envisioned for other vaccination campaigns.
5.1.4. Primary prevention and health promotion programmes
The SPF runs the major national information campaigns and health promotion services, for instance, tobacco cessation services (https://www.tabac-info-service.fr/), nutritional and physical exercise campaigns (https://www.mangerbouger.fr/) and information campaigns for expecting parents and parents of newborns (www.agir-pour-bebe.fr).
Implementing a health promotion and prevention policy throughout the life-course was one of the first priorities of the French National Health Strategy for the years 2018–2022, a strategic document setting health system priorities (MoH, 2017). The subsequent prevention plan targeted different population groups (MoH, 2019c). For infants measures focused on the perinatal period (reducing alcohol, smoking and drug use in pregnancy and introducing postnatal home visits). For children and adolescents measures mainly targeted obesity (for instance through food education in schools), risky sexual behaviours and addictions (easier access to outpatient clinics for young substance users). For the adult population the plan focused on tobacco consumption by providing extensive SHI coverage of smoking cessation treatments. The national prevention plan also introduced measures for improving access to preventive care for individuals with reduced autonomy, such as systematic annual medical and dental check-ups in residential institutions for the elderly and for people with disabilities (MoH, 2019c). Nevertheless, the investment in the national prevention plan remains modest – €400 million over five years (CIS, 2018).
In 2017 a specific fund was created to prevent tobacco smoking, to help smokers quit and to finance research on tobacco policies. Taxes on cigarettes have also significantly increased since 2017 (Order of 6 November 2017). Prevention of alcohol abuse consists mainly of public campaigns in the general population with also a focus on reducing alcohol consumption during pregnancy (MILDECA, 2018). Measures promoting physical activity remain limited to legally enforced prompts for physical activity in commercials for soft drinks and food with added sugar, salt or artificial colourants, since 2007 (Order of 27 February 2007). Furthermore, since March 2017 GPs can prescribe physical activity to patients suffering from diabetes, heart problems or cancer (Decree no. 2016-1990 of 30 December 2016). The efficiency of prescribed physical activity for these groups is under evaluation before generalizing the policy more broadly. One of the most important investments in promoting healthy food choices includes a front-of-pack scoring system for food products, the Nutri-Score, which rates the calorie, sugar, salt, saturated fat, fibre and protein content of packaged products from A (best nutritional quality) to E (worst nutritional quality). This rating became mandatory for all food commercials in 2021. Food manufacturers may, however, opt out from this obligation by paying a fee to the SPF (National Assembly, 2019).
Despite an increasing political focus, France ranks low for spending on health promotion and prevention among OECD countries (OECD, 2021b). In 2019 only 1.9% of health expenditure was spent on organized prevention, compared to 3% on average in the EU (OECD, 2021b). The historical orientation of the French health system towards curative medicine was identified as a major constraint for developing effective prevention strategies during the Covid-19 pandemic (Borowczyk & Ciotti, 2020). It has also been recognized that the medical curriculum could be strengthened by integrating more training in disease prevention. Therefore, since 2018 all students on health-related training tracks (including medicine, dentistry, nursing, midwifery, physiotherapy and pharmacy) have to participate in three months of health promotion and prevention activities, such as health-related workshops and information campaigns in schools, workplaces, nursing homes and prisons (MoH & Ministry of Higher Education and Research, 2018c).
As of 1 July 2025, smoking will be banned in designated outdoor public spaces, including beaches, public parks and gardens, bus shelters, and vicinity of schools, libraries and sports facilities. Those in violation of this ban will face a €135 fine. This new regulation builds upon existing bans that already prohibited smoking in enclosed public areas such as government offices, businesses, indoor cafés and restaurants, public transport and educational institutions, as well as at children’s playgrounds and in private vehicles carrying minors.
This measure is part of France’s broader effort to reduce tobacco use and better protect children and adolescents by reducing exposure to secondhand smoke. Tobacco consumption remains a significant public health concern in France, responsible for around 75,000 deaths each year. This ban also aims to protect the environment, particularly by reducing litter from cigarette waste, as an estimated 20,000 to 25,000 tons of cigarette butts are discarded annually.
Authors
Since January 2024, and after pilot testing in the Hauts-de-France region, physicians, nurses, midwives, and pharmacists can provide prevention consultations to their patients, which are fully covered by the national health insurance fund (CNAM) for a tariff of €30 in mainland France and €31.50 in overseas territories whatever the professional involved. These consultations, which can last on average between 30 and 45 minutes, target specific age groups (that is, 18–25, 45–50, 60–65, and 70–75 years old). They allow taking stock of lifestyle habits (for example, nutrition, sleep, physical activity, addictions, mental and social well-being, sexual health, and immunization), and providing advice tailored to patient age and individual situation. At the end of the consultation, a personalized individual prevention plan is issued and sent to the referring general practitioner of the patient. Currently, communication campaigns to raise awareness of this new scheme are ongoing, while a specific strategy is being devised to reach vulnerable population groups, including those with the fewest contacts with the healthcare system. Ultimately, the goal is for every French person to have access to four of these consultations over the course of their lifetime.
More information (in French):
https://sante.gouv.fr/actualites/actualites-du-ministere/article/mon-bilan-prevention-fait-campagne
5.1.5. National screening programmes
Three national cancer screening programmes are in place in France: for breast, cervical and colon cancer (MoH, 2018d). These screening programmes have been established by the INCa, a scientific expertise and coordination agency dedicated to cancer under the umbrella of the MoH and the Ministry of Higher Education and Research. Since 2004 all women between 50 and 74 years old are invited for a mammogram and a clinical examination with a radiologist, free of charge, every two years (INCa, 2017). Moreover, since 2009 all adults aged between 50 and 74 years are systematically invited to colon cancer screening every two years (INCa, 2021a). The screening programme for cervical cancer, implemented in 2018, offers a smear test every three years to all women aged between 25 and 30 years and every five years for women aged 31–65 years (INCa, 2021b). The rate of timely access to cervical cancer screening for women in France is estimated to be 82%, compared to 73% on average in OECD countries (OECD, 2019d). Screening for other types of cancer, such as skin cancer, is at the discretion of patients and GPs. The 10-year ambitions of the new Cancer Plan (2021–2030), include improving screening adherence (from 9 to 10 million tests per year), reducing avoidable deaths by 50 000 cases per year, improving survival of patients with the poorest prognoses, and ensuring equity in access to the newest cancer treatments. The new plan has received €1.7 billion over five years to attain these objectives, which is 20% more compared to the previous Cancer Plan (2016–2021) (INCa, 2021c). However, a recent public evaluation suggested that, despite the investments made over the past two decades, cancer screening rates have slightly dropped, notably owing to geographical and social difficulties in accessing preventive services and the inefficient use of dedicated funding (Dupays, Leost & Le Guen, 2022).
Screening and follow-up of pregnant women is mainly provided by self- employed GPs, gynaecologists and midwives, or gynaecologist-obstetricians. The follow-up is 100% reimbursed by the SHI and includes seven medical consultations, a minimum of three ultrasounds, and screening of maternal health and risk behaviours (such as tobacco and alcohol consumption). Prescription of folic acid, assessment of protein and glucose in the urine, urinary tract infections, and antibodies against high-risk infections and Down syndrome are also systematic, and covered 100% by the SHI (CNAM, 2021q; HAS, 2016).
5.1.6. Organization of occupational health services
In France occupational health and safety involves several actors and has undergone important changes over the past decade. The latest reform, part of the August 2021 law, aimed to reinforce prevention and modernize occupational health and prevention services (Law no. 2021-1018 of 2 August 2021). It reinforces the responsibility of employers to guarantee employees’ physical and mental health at work and to prevent work-related accidents, illnesses and psychosocial risks via information, training and workplace arrangements. This law also gives more weight to employees’ representatives for improving employees’ well-being and safety in the workplace. Employers have the obligation to provide occupational health and prevention services. Large firms finance and host their own occupational health services, whereas smaller firms work with external health services. Occupational physicians have the mission to monitor employees’ health status and ability to do their job and to ensure that their physical and mental health is not altered by their work. In practice, the number of occupational physicians has strongly diminished over time due to the lack of attractiveness of this specialty for physicians (Chastel, Blemont & Siahmed, 2017). In parallel, a number of new occupational health professions have been developed, such as occupational health nurses and prevention experts, coordinated by occupational physicians. E-health solutions are also increasingly supported (Decree no. 2022-679 of 26 April 2022). While occupational prevention and health services are well developed, and it is mandatory for employers to provide such services to their employees, there are no equivalent services for self-employed workers.