-
08 December 2025 | Country Update
France increased flat co-payments to reduce its budget deficit
3.4. Out of pocket payments
Given the importance of co-payments left to patients by the SHI, 96% of the French population held CHI in 2019 (Pierre & Rochereau, 2022). Therefore, in 2019 France had the second lowest share of OOP spending in total health expenditure (around 9%) amongst OECD countries (after South Africa at 8%) (OECD, 2021b). On average, OOP costs accounted for 2% of final household expenses in 2019, compared to 3% among all OECD countries (OECD, 2021a). This OOP spending corresponds to the cost of care directly paid by households without counting the premiums paid for private CHI. It is estimated that in 2017 private payments including these premiums accounted for 4% of household budgets but could reach 8% for the lowest income groups (Fouquet & Pollak, 2022).
Overall, the share of direct OOP costs in current health expenditure has been stable and decreased slightly over the past decade, from 10% in 2010 to 9% in 2019 (OECD, 2021b). The reduction in OOP costs related to hospital care appears to be partly driven by the ageing of the population, leading to an increase in patients covered by the ALD scheme for chronic diseases reducing cost-sharing. In the ambulatory sector the caps applied to extra-billing in recent years (see section 3.7.2) and higher reimbursement rates applied to certain drugs, including hepatitis C treatments and nicotine substitutes, have also contributed to reducing OOP payments (DREES, 2020a). In 2020 the Covid-19 pandemic and related restrictive measures led to a significant reduction in the use of all types of care, and, in particular, a lower use of hospital services for non-urgent conditions, which resulted in a drop in OOP payments as a proportion of all health consumption by 6 percentage points between 2019 and 2020 (DREES, 2020a).
In 2020 the majority of OOP spending was on LTC (43%), followed by pharmaceuticals and therapeutic devices (26%), outpatient care (26%) and inpatient care (5%) (OECD, 2021a).
3.4.1. Cost-sharing (user charges)
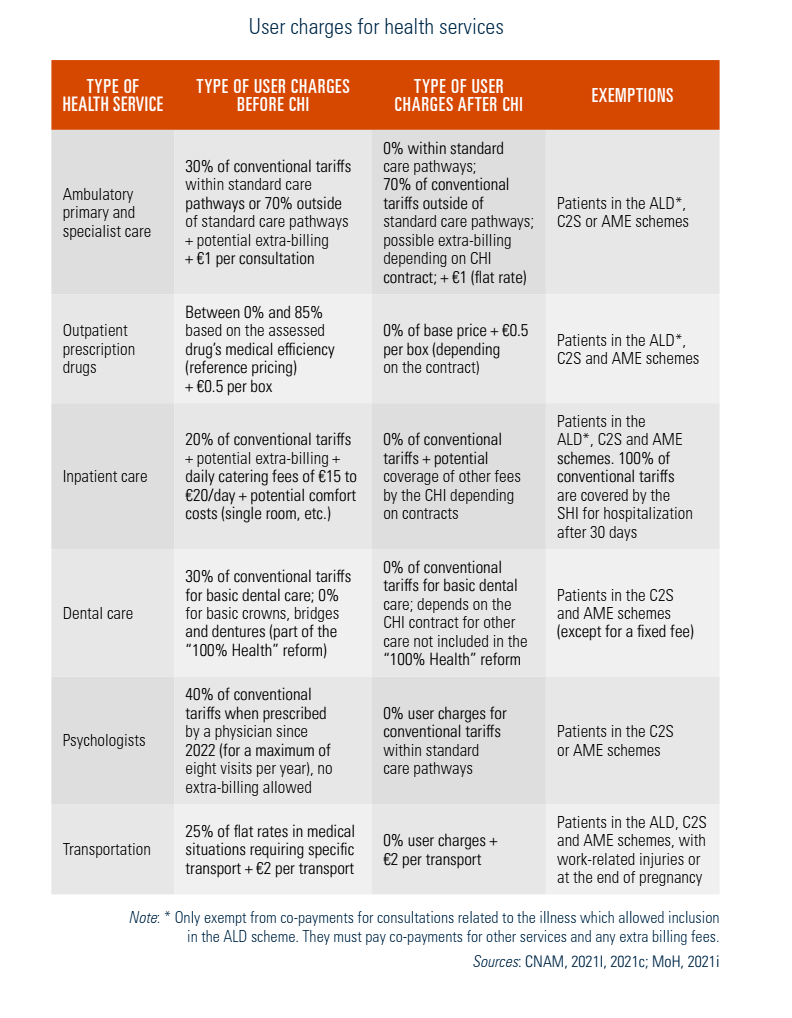
User charges are asked for most health care goods and services in France. Primarily, patients are asked to pay a proportion of the tariffs (Ticket modérateur) or the full price to be reimbursed later by the SHI (Table3.4). Cost-sharing arrangements, initially intended to reduce inappropriate demand for care, are also used increasingly to encourage patients to follow standard care pathways (see section 5.2). However, given the high proportion of the population with CHI, which sometimes reimburses OOP payments as a third-party payer, the impact of cost-sharing on patients’ behaviour appears to be limited. Therefore, over time different types of flat deductibles have been introduced to encourage patients to consider the costs of treatments and to contain demand for targeted services (Table3.4).
Table3.4
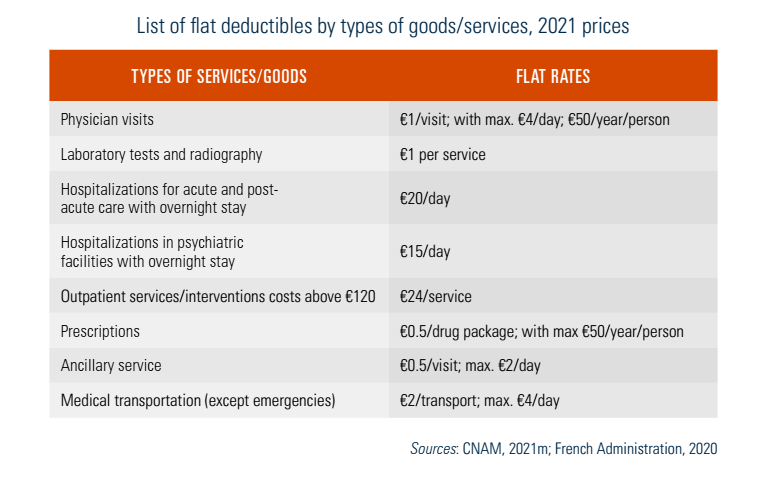
Flat rates, or deductibles (Participation forfaitaire), apply to outpatient consultations, pharmaceutical products, medical transportation, and consultations and care from allied health professionals. Overnight hospitalizations are subject to a daily catering fee (Forfait journalier); this does not apply to hospitalizations at home or to day hospitalizations. In 2020 this fee amounted to €20 per day for acute and post-acute rehabilitation care and €15 per day for psychiatric hospitalizations (Adjerad & Courtejoie, 2021b). The hospital fees are regularly reimbursed by CHI, but the deductibles for outpatient consultations and prescriptions are, in principle, not reimbursable by the CHI.
A complex capping system has been introduced concurrently to flat deductibles. Per service, per day, and annual caps have been introduced to limit financial consequences for consumers. Nevertheless, by their nature, these deductibles (which are not adjusted by income) pose the risk of inducing inequity in access to care. While they have limited effects on the behaviour of higher-income groups, they can be an important barrier for those with low income. Direct cost-sharing expenses could be particularly significant for older patients, as they are more likely to need longer hospitalizations, and patients without a CHI contract, especially in post-acute rehabilitation and in psychiatric hospitals, where the average length of stay is longer (Adjerad & Courtejoie, 2021b).
Given the level of cost-sharing, specific measures exist to limit the OOP costs of populations with very low revenue and certain patient groups with high health care needs (Table3.5). Populations exempt from cost-sharing include pregnant women in their third trimester, persons with a disability pension, persons with complementary solidarity insurance due to their low revenue (C2S), as well as persons covered by the ALD scheme (see section 3.3.1). There is also a cap for user fees for hospitalizations, limited to 30 consecutive days, which applies to all patient groups. This cap does not include daily catering fees for hospitalizations, which can lead to significant OOP payments for people without CHI (Adjerad & Courtejoie, 2021b). However, there are a number of situations for which the SHI also covers the catering fees, for instance, pregnant women during the last four months of pregnancy, persons covered by the complementary solidarity insurance (C2S), veterans and persons covered by the AME.
Table3.5
Despite these measures, the top 1% of patients with the highest OOP payments for acute hospitalizations paid on average €5540 per year in 2016 (Adjerad & Courtejoie, 2021b). A part of this amount was paid by the CHI, but there are no data on the final OOP payments for patients and their distribution by income categories. Patients with high hospital OOP expenditures (before CHI payment) are on average older, accumulate several short-term hospitalizations, and approximately half (54%) have a chronic illness, suggesting that the ALD scheme is not sufficient for reducing extreme OOP costs related to hospitalizations (Adjerad & Courtejoie, 2021b).
Under strong pressure to reduce the public health deficit, the French Government increased flat co-payments and medical deductibles for patients in March 2024. The deductibles were doubled: from €0.50 to €1 per box of reimbursed medicines and per paramedical act; from €1 to €2 for medical consultations, procedures and laboratory tests; and from €2 to €4 for medical transport. These deductibles cannot be covered by complementary health insurance (CHI). However, there is an annual cap on these user charges which remained at €50 per person. Moreover, patients under 18, pregnant women, and beneficiaries of the complementary health insurance scheme for individuals with low income or state medical aid for undocumented migrants remained legally exempt from these charges.
As part of preliminary budget discussions for 2026, the government proposed in October 2025 a second round of increases, doubling the fixed payment for boxes of reimbursed medicines to €2, medical transport to €8, and medical consultations to €4, with a higher annual ceiling. However, both patient and health professional organizations, as well as the board of the National health insurance fund, strongly opposed this proposition, arguing that this would disproportionately affect people with chronic conditions and low-income households, and that it could lead to delayed or forgone care.
Following fierce public and political opposition, the government abandoned the planned increase in early December 2025. As a result, alternative sources of funding proposed by the government include a temporary contribution from CHI providers and an increase in earmarked tax adjustments.
Authors
3.4.2. Direct payments
Health care in the ambulatory sector has traditionally been paid upfront by patients before being reimbursed by the SHI. This system has been gradually transformed, and third-party payment is now common for pharmaceuticals and medical devices (including eyewear and audio prosthesis), as well as for laboratory tests. It is also systematically applied for specific patient groups, including those in the ALD scheme, benefiting from the complementary solidarity insurance (C2S) or the state-funded medical aid (AME) scheme, as well as for patients who had a work-related accident. It is also systematically applied in specific types of care, including maternity care, contraception for women aged up to 25 years, as well as in national screening programmes. OOP payments covered by CHI are subject to direct payment to different extents. Increasingly, health care providers choose to collaborate with CHI providers and bill them directly to avoid direct payments for patients. However, this practice varies depending on the patient’s CHI contract provider and the health care provider.
The costs of inpatient hospital services are directly paid by the SHI, and CHI if the patient has it. Outpatient hospital visits are paid similarly to consultations in the ambulatory sector.
3.4.3. Informal payments
Informal payments are rare in France, and health care providers engaging in these practices are subject to disciplinary sanctions. According to the Eurobarometer survey on corruption, 5% of French patients had to give a gift, favour, extra money or a donation to a public health care practitioner (doctor, nurse or hospital) for receiving services in 2019, which is around the EU average (5%) (European Commission, 2020b).