-
03 April 2017 | Country Update
An open access online platform to facilitate reporting of adverse events
2.8. Regulation
The French health care system was initially organized according to a Bismarckian model of provision and payment for health care. However, it has developed into a mixed Beveridge and Bismarck model, characterized by an almost single public payer, the increasing importance of tax-based revenue for financing health care and strong state intervention. SHI is financed by employer, employee and retiree contributions, increasingly substituted by earmarked income taxes. Providers of outpatient care are largely private, while hospital beds are predominantly found in public or private non-profit-making hospitals.
In the context of increasing health care expenditure, the increasing deficit of SHI and the overall social security system, the role of the state in steering the system through regulation has increased since the early 1990s. Regulation, therefore, involves negotiations among provider representatives (hospitals and health professionals), the state, represented by both the ministry in charge of health, the ministry in charge of the budget and public accounts, and SHI. The outcome of these negotiations is translated into administrative decrees and laws passed by the parliament. These include public health acts and acts related to social security funding and reforms.
The Directorate of Social Security proposes an annual Social Security Finance Act, which is debated and then approved by the parliament. This Act establishes the provisional health care budget, or rather the expected ONDAM (see section 3.3.3). Because in France providers are mostly paid by FFS and a per-case basis retrospectively, ensuring that SHI health expenditure will match the (approved) national ceiling for SHI expenditure is difficult (see section 3.3.3). Indeed, the ministry in charge of health approves statutory tariffs but does not control volume as there is still freedom of choice and no limitation of utilization of services. However, regulatory mechanisms such as semi-gatekeeping with financial incentives and non-refundable deductibles on physician visits, drugs and ambulance transportation (see section 3.4.1) can be seen as attempts to regulate volume by using price sensitivity.
An open access platform managed by the French Ministry of Health
has been made available online in March 2017 to facilitate access to
the different reporting systems of adverse events (http://social-sante.gouv.fr/grands-dossiers/signalement-sante-gouv-fr).
Those include: adverse effects of medical products (such as drugs or
medical devices), medical procedures, and products of daily life (such
as food supplements, cosmetics or cleaning agents). Through the new
platform and depending on the type of adverse events, health
professionals and patients will be able to directly report such events
on the platform, be directed towards pre-existing electronic reporting
systems (such as the platform dedicated to adverse effects of
radiotherapy) or be informed about specific procedures for events which
can only be notified by specialized health professionals. This new
measure, aiming to increase the quality and safety of the French health
system, was planned in the 2016 Health Reform Law (Loi n°2016-41 du 26
janvier 2016 de modernisation de notre système de santé).
More information (in French): http://social-sante.gouv.fr/actualites/presse/communiques-de-presse/article/ouverture-du-portail-signalement-sante-gouv-fr
Authors
2.8.1. Regulation and governance of third-party payers
SHI
SHI schemes are under the supervision of the Directorate of Social Security. In order to ensure that SHI measures will meet the objectives of the government health policy, SHI schemes sign a triennial contract with the ministry in charge of health defining the objectives, the management and the governance of SHI. The objectives of this agreement are: to improve efficiency in the management of SHI, reduce inequities in access to health care services and develop risk management. Actions to meet these objectives set forth in the 2014–2017 agreement on objectives and management include developing good quality patient care pathways.
UNCAM (see section 3.3.3) represents the SHI funds in negotiations with the state and health care providers. The director-general of UNCAM is also the director of CNAMTS. The director-general is appointed by the government, and the executive power of this position has been strongly reinforced at the expense of the UNCAM board, whose role is now limited to strategic matters. Collective agreements with doctors and other organizations of professionals in private practice are negotiated and signed by the director-general alone, illustrating the withdrawal of employee and employer unions from the management of SHI. SHI is, therefore, fully responsible for the economic consequences of the agreements that it negotiates and signs, for example with health professionals in private practice. SHI can also set the level of user charges, although this power is limited to a certain extent by the political acceptability of the proposals.
VHI
There are three types of VHI suppliers (see section 3.3.2), which operate under three different sets of regulation: the mutual insurance companies are regulated by the mutual insurance code, the commercial insurance companies are regulated by the commercial insurance code, and the provident institutions are regulated by the social security code. All three types of VHI suppliers fall under the supervision of the Prudential Control and Resolution Authority (Autorité de contrôle prudentiel et de résolution).
VHI suppliers participate in the governance of the health care system through the National Union of Complementary Health Insurance Organizations (Union nationale des organismes d’assurance maladie complémentaire), which is consulted prior to the annual Social Security Finance Act and all health care reforms, in particular when they are related to health care system financing. It is also consulted prior to changes on SHI coverage rate and prior to the introduction of new products in the SHI benefit package and participates in the negotiation of national agreements with health care professionals. As a member of the pricing committee, the Economic Committee for Health Products (Comité èconomique des produits de santé; CEPS), the National Union participates in the negotiation of drugs and medical devices prices, along with representatives of several ministries and SHI.
2.8.2. Regulation and governance of providers
Professionals
Professionals practise under the regulations of the public health code, which includes all regulations related to patient and professional rights with respect to medical goods and health services, planning the provision of out-of-hospital services and ensuring coordination between hospital and ambulatory care. In France, roughly two-thirds of practising health professionals are independent self-employed providers. Despite recent regulations aiming to plan geographical distribution of doctors, they retain the freedom to establish their practices where they wish (see section 6.1.3).
The National Union of Health Professionals is the single organization that can legitimately negotiate with the payers at the national level on behalf of all types of self-employed independent health professionals. It is consulted annually by SHI and VHI representatives on matters related to the organization of the health care system and health professions, such as the relationship between office-based and hospital physicians, demography of medical professions, access to care, continuing medical training and regulation of health care expenditure. At the regional level, regional unions of health professionals negotiate with the ARSs (see section 2.4).
There is no formal recertification or relicensing process. However, in order to ensure lifelong quality of practice of health professionals, doctors, midwives, dentists, pharmacists, biologists, nurses, physiotherapists and podiatrists must undergo DPC. Within the DPC process, accreditation exists for a limited number of high-risk medical specialties (i.e. specialties with a high medical risk for the patients). It is optional and concerns physicians or medical teams practising in hospitals. Medical specialties involved include obstetrics and gynaecology (including ultrasound imaging), surgery, interventional radiology, anaesthesiology and other interventional specialties such as cardiology. Accreditation permits physicians to claim a deduction on the premium they pay for their professional insurance. The accreditation process includes a registry of adverse events, use of practice guidelines and review criteria and participation in educational sessions in risk reduction.
Hospitals
Both human and physical resources of hospitals are controlled by the government through different mechanisms. The ministry in charge of health, thorough the HAS, ensures that public and private hospitals and hospital physicians meet standards of competence through a certification process every four years.
Certification is a two-step process. First, a self-appraisal is conducted by hospitals based on HAS guidelines. It requires the compilation of a large amount of information, particularly with respect to quality indicators. Second, a team of experts assigned by HAS visits the hospital and undertakes the certification review.
Hospital quality assurance and risk management are monitored by the ministry in charge of health through Scope Santé (http://www.http://www.scopesante.fr.fr). Hospital quality indicators are also compiled through the Coordination for the Measurement of Hospital Performance and Improvement in Quality of Care (Coordination pour la mesure de la performance et l’amélioration de la qualité hospitalière). Experimentation with financial incentives has been ongoing since 2012 under the programme of financial incentives to improve quality (incitation financière à l’amélioration de la qualité). Moreover, in the field of rare diseases, France has developed dedicated centres.
2.8.3. Registration and planning of human resources
At the national level, the number of doctors, and to some extent their areas of specialization, is regulated by the numerus clausus, which is set by the government annually and controls access to the second year of study in medical schools. This numerus clausus is then applied at the regional level, taking into account current inequalities in the geographic distribution of doctors. There is also a numerus clausus limiting the entry of students in other health professions, such as nursing, midwifery, dentistry, speech pathology and physiotherapy.
Registration by their professional association (see section 2.3.6) is mandatory for practising doctors, pharmacists, dentists, midwives, physiotherapists and nurses. It is usually granted upon request after the initial training and it is good for life. Moreover, registration in the national information system on health professionals (ADELI) in the ARSs is also mandatory for almost all health professionals.
2.8.4. Regulation and governance of pharmaceuticals
Before being put on sale, all drugs must obtain market authorization (autorisation de mise sur le marché; AMM) either at European or national level. This specifies the conditions for the prescription and supply of drugs for which a medical prescription is mandatory and identifies drugs that are subject to special prescription rules (see section 5.6.3).
In order to qualify for SHI coverage, a drug must be included in the so-called “positive list” of reimbursable drugs established by ministerial decree on the advice of the HAS Transparency Commission (see section 2.7.2) and the CEPS pricing committee.
In order to be included on the positive list, evidence must be supplied of the SMR for the drug (see section 2.7.2). The coverage and level of coverage is determined by decree based on the SMR and the seriousness of the condition (Table2.1). However, drugs that lead to lower cost of treatment can be covered despite the fact that their SMR is insufficient.
Table2.1
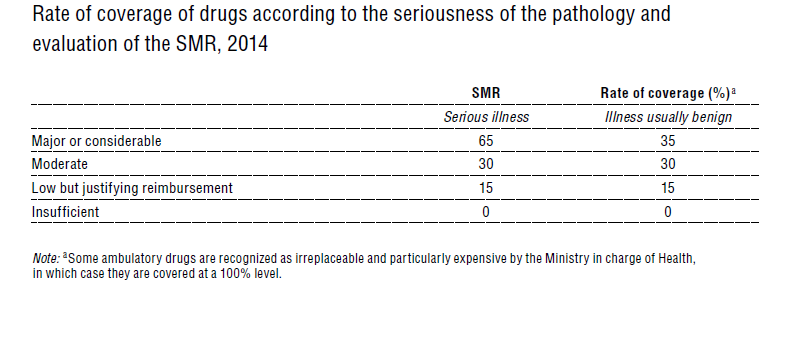
The vast majority of drugs are covered at a 65% rate. In 2011, among the 240 new drugs examined, 191 were found to justify 65% coverage.
In addition to the SMR, the Transparency Commission evaluates the ASMR in comparison with available treatments or drugs already available for the same pathologies (see section 2.7.2).
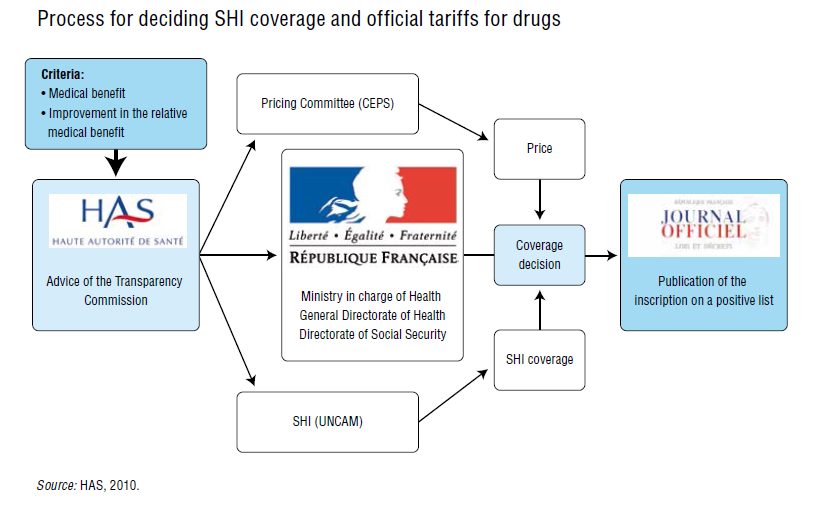
The drug price, which serves as the basis for reimbursement, is then set through a bargaining process between the CEPS and the manufacturer, using an international benchmarking procedure for the most innovative products.
CEPS is an interministerial committee defined by decree (article D162-2-1 of the social security code). It is composed of representatives of the ministers in charge of health, of the economy and of research, plus representatives from SHI and complementary health insurance organizations. According to the social security code, the price must be set according to the ASMR, the price of other drugs with the same therapeutic indications and the estimated volume of sales. Drugs offering a therapeutic advance can have a price higher than the reference, whereas drugs classified with no relative medical benefit (ASMR group 5) would get a statutory tariff, and so be subsequently covered only if their price is lower than that of their alternatives. Since 2003, a new procedure has allowed the manufacturer to propose a price that is consistent with prices already defined in four other European countries (the United Kingdom, Germany, Spain and Italy); the procedure was initially limited to ASMR groups 1 and 2 (major and important improvement) products but has now been extended to ASMR 3 and certain 4 (low and minor improvement) drugs as well; it is worth noting that the manufacturer may nevertheless opt for the standard bargaining process. Drug coverage and pricing processes are summarized in Fig2.2.
Fig2.2
Depending on their level of toxicity or risk of inappropriate use, medicines are classified in the public health code based on different categories that will determine their prescription rules and facility of access. Drugs that fall into the category that does not require a prescription can currently only be sold in pharmacies. The distribution of drugs is closely regulated, both for wholesalers and for pharmacies. Wholesalers (grossistes-répartiteurs) have a public service mission and fall under the regulatory control of the ANSM. They are regulated in terms of the range of drugs supplied, level of stock, territory, delivery time and mark-ups. Since January 2012, the mark-up is 6.68% for manufacturer prices below €450 and 0% for prices above €450.
Pharmacies have a monopoly on the dispensing of medicines. Generally, retail pharmacies must be owned by a qualified pharmacist or by a group of pharmacists associated within a company; these pharmacists or companies cannot be proprietors of more than one pharmacy. As an exception to this rule, mutual insurance associations and the SHI scheme for miners may also own retail pharmacies. The number of pharmacies is regulated by a numerus clausus that takes into account both the size of the population to be served and the distance to the nearest pharmacy. Pharmacists have financial incentives to deliver generic drugs (see section 3.7.1).
Direct-to-consumer advertising for drugs is subject to prior authorization and is restricted to specialties that meet three criteria: they can be delivered without physician prescriptions; they are not covered by SHI; and no restriction on advertisement has been included in the AMM of the product. Vaccines are the only exception to this rule. Since 2012, advertisements directed at health professionals are also subject to prior authorization and are prohibited for health products that are undergoing a risk–benefit re-evaluation.
Internet sales of non-prescription drugs have been authorized since 2013, but uptake has been very limited because of the significant regulatory burden in establishing an online sales presence. Only pharmacists are eligible to engage in this activity, which must be directly linked to a physical pharmacy and authorized by the ARS.
All drug-related adverse events must be reported by physicians, dentists, midwives and pharmacists to the regional centre for pharmaceutical vigilance (Centre régional de pharmacovigilance), which is responsible for making the necessary inquiries and notifying the manufacturer. The ANSM oversees and coordinates the national system for pharmaceutical vigilance. Since 2011, patients and patient associations may directly declare adverse events. Validated reports of adverse events must be reported to the European Medicines Agency within 15 days. Moreover, ANSM inspectors have a key role in the fight against counterfeit pharmaceuticals, in collaboration with customs inspectors, the Ministry of Justice, the police and the gendarmerie. In the event of suspected fraud, drugs may be subject to recall or quarantine.
2.8.5. Regulation of medical devices and aids
The market for medical devices is more loosely regulated than the markets for drugs or major medical equipment, particularly in terms of quality and safety standards. Compliance with quality and safety standards is assessed by the provider for devices that present a very low risk for the patient (medical beds, stethoscopes, etc.). Other devices must be assessed by an independent body selected by the manufacturer (to obtain a European conformity (Conformité Européenne) mark). Monitoring of the market is under the responsibility of the ANSM.
The CNEDIMTS advises the ministry in charge of health, which decides whether to include a device in the positive list based on its medical benefit rating. It also advises CEPS regarding pricing, which will depend on the ASA (see section 2.7.2). In this sector, the market price generally is not fixed; rather, the SHI statutory tariff is negotiated with the manufacturer and then is used as the basis for reimbursement. As a result, there is a high level of extra-billing for medical devices. Medical devices and prostheses are subject to various rates of coverage depending on the device. In certain cases (e.g. spectacles, dentures, hearing aids), the levels of coverage are particularly low.
2.8.6. Regulation of capital investment
The ARSs are generally responsible for planning services and for the authorization of hospitals as well as for changes to the existing hospital infrastructure, including restructuring and mergers. The overall strategy for capacity and investment planning is mainly implemented through SROSs and the related target contracts (contrats d’objectifs et de moyens; see section 2.5.1). Target contracts form a regulatory framework that is explicitly designed to implement changes; this framework applies equally to all hospital facilities that fall within the health care sector. The only exception is the construction of (new) hospitals (private and public) and comprehensive emergency centres, which must be authorized by the ministry in charge of health. The ARS also delivers authorizations for the implementation of major medical technologies (see section 2.5.3).
There is a large body of legal rules controlling the building and operation of hospital facilities, covering infrastructure and equipment. All the relevant texts are referenced in a guide that is published by the ministry in charge of health.
Depending on the specific sector and public health priorities, capital investments in the health care sector are either covered by payments for service delivery or funded by specific national or regional programmes (see section 4.1.1). The ANAP (see section 2.3.3) oversees and audits hospital investments and reorganizations in the health and social care sectors; it also provides expertise to the central administration and to the ARSs.