-
26 January 2024 | Country Update
An expert group outlines a plan on hospital and emergency services network reform -
01 December 2022 | Policy Analysis
Efforts to improve integration of care
5.4. Specialized ambulatory care / inpatient care
Specialized care, both ambulatory and inpatient, is provided by five types of public organization. Four of these are owned by the hospital districts and one is owned by one or more municipality.
- Five university/tertiary hospitals that are attached to medical schools and serve as central hospitals for their immediate population. Their tertiary service catchment populations range from 741 807 (Oulu) to 2 148 143 (Helsinki) (Kuntaliitto, 2018a). For selected treatments and population groups, their responsibilities may be nationwide.
- Central hospitals (15 overall, in addition to the above-mentioned university hospitals). These hospitals provide the traditional range of medical specialties with some subspecialization in surgery and internal medicine. They all maintained emergency and surgery services on a 24/7 basis until 2018, but Government centralization efforts have reduced the number of central hospitals that provide a broad spectrum of services to eight, located in Lappeenranta, Lahti, Jyväskylä, Joensuu, Rovaniemi, Vaasa, Seinäjoki and Pori. The catchment populations for these central hospitals range from around 100 000 to 200 000. Central hospitals with a more limited variety of on-call services are in Hämeenlinna, Kemi, Kokkola, Kajaani, Kotka, Mikkeli and Savonlinna. These hospitals have population bases ranging from 43 000 to approximately 170 000. The Government is currently preparing to change the Vaasa central hospital back to a broad spectrum hospital.
- Hospital districts previously operated smaller local hospitals, but many of them have either been shut down or merged into university or central hospitals. Examples of such hospitals are located in Turku, Tampere and Oulu University Hospital catchment areas. These previously fairly independent hospitals are currently run as university clinic departments. Typically, the range of inpatient care is limited to the largest specialties, such as surgical day care, and out-of-hours services are variable. Catchment populations may range from 20 000 to 100 000. As well as the main hospitals located in Helsinki (Helsinki University Central Hospital, HUCH), Helsinki University Hospital district operates four, at least nominally, independent hospitals and two subsidiary hospitals of HUCH in Espoo and Vantaa. The overall number of hospitals in this category is currently 13 and their population bases range from 43 000 to more than 200 000. Their profiles are, in some cases, shifted to primary care or rehabilitative service provision with closure of specialist on-call services.
- Hospital districts own psychiatric inpatient facilities located at a distance from the central or other somatic care hospitals. These hospitals have either been closed (11 since 2012), or there are plans to close them (six hospitals). Their current number is 10. Some of them have outpatient departments, but ambulatory psychiatric care is mostly provided by departments at central or university hospitals.
- Specialist-run health centre hospitals (14 overall), owned and run by single municipalities (in larger cities) or jointly by several municipalities, mostly provide primary care but with some basic internal medicine and surgical services in ambulatory and day surgery settings. Their future is uncertain, as some may be undergoing conversion into inpatient health centre units, and some have rented part of their premises to private companies.
The number of patients treated in specialized somatic and psychiatric care has increased steadily in recent years. In theory, all patients admitted to secondary or tertiary care need a referral from primary care. In 2015, 41% of all inpatient care episodes were referred from the health centres, with a further 18% referred by private providers. However, a large share of patients bypass initial referral by directly accessing hospital-based emergency care units (THL, Sotkanet.fi). The percentage of in-hospital care periods beginning through emergency departments is particularly high in the north-eastern parts of Finland (Fig5.2).
Fig5.2

Since 2014, patients have been able to choose where they want to receive specialist services (Health Care Act 2010). The referring physician must discuss the options with the patient and offer information regarding, for example, waiting times. Waiting times for specialist services can be lengthy (see section 5.2), particularly for orthopaedics, gynaecology and ophthalmology.
The quality, outcomes, performance and efficiency of the Finnish hospital system has been studied extensively (EuroHOPE Study Group 2014; Kittelsen et al., 2015). Recommendations to develop a focus on quality was an MSAH priority when the 2010 Health Care Act (1326/2010) was issued with a section (§8) on quality and patient safety. The Association of Finnish Local and Regional Authorities published guidance on the implementation of this legislation (Koivuranta-Vaara, 2011). The University Hospitals employ dedicated chief medical officers to supervise the development of quality and patient safety in their catchment area.
Vertical and horizontal administrative integration brought by the ongoing Health and Social Care Reform is expected to ensure that people who need integrated services are identified, their service and care chains and packages are defined, health and social welfare services are coordinated with other services provided by municipalities (for example, education, unemployment services), and information about clients exchanged between different providers. In addition, there are recommendations based on the national Care Guidelines (Nuutinen, 2017) and adapted at the county level, that address integration of primary and secondary levels of care, and outline patient pathways.
Despite these efforts, a lack of continuity of care between different parts of the system remains. A specific bottleneck is the point of discharge from hospital care for patients who no longer need specialist care but lack suitable follow-up care at their place of residence. Consequently, in some health authorities, dedicated teams of nurses, coordinated by a primary care physician, have been established to ensure patients’ safe return home. These teams can also include physiotherapist and occupational therapist, and the follow up may include a short intensive home rehabilitation period.
5.4.1. Specialized ambulatory / outpatient care
Specialized ambulatory care is mainly provided in outpatient departments of public hospitals, or, for minor treatments and where expertise is available, in larger health centres. The latter may collaborate with their local or central hospitals for the acquisition of consultative services and small procedures, such as endoscopy and stress ergometry. Over time, the total number of outpatient appointments per 1000 population has increased from 1022 in 2006 to 1401 in 2016.
Private clinics offer services, particularly in the areas of gynaecology and ophthalmology, but also for other specialties depending on regional demand. The clinics can be partly or wholly owned by a publicly financed hospital district or a private insurance company, but for-profit companies prevail. The NHI reimburses part of the cost when patients use private ambulatory specialist services. The number of privately provided visits in 2017 was 2.7 million, corresponding to a ratio of 0.5 per inhabitant. The reimbursement covered on average 16% of the total cost (Kela, 2018b).
5.4.2. Inpatient care
Inpatient care is provided largely by hospital districts, but there are also large private hospitals specializing in orthopaedic surgery (2 hospitals), cardiology (1), cancer care (1) and some smaller units (see Chapter 4). Inpatient care has been transformed since the early 1990s towards more centralized services, as well as a shift into other settings. This is reflected in a reduced number of hospitals, a decreased number of inpatient care periods, a shortened average length of stay, and an increase in day surgery. Many inpatient wards have been closed or combined with other general-purpose wards, as outpatient care caters for most needs. This is especially true for some specialties, such as pulmonology, rheumatoid diseases and dermatology.
Several publications have shown that there have been unacceptable levels of regional variation in surgical procedure rates and medical care in Finland (Keskimäki et al., 2000; Vuorma et al., 1998; Mikkola et al., 2005; Nguyen et al., 2003). Together with the long waiting times for elective surgery, the persisting rates of variation resulted in the instigation of a national project called “Care Guarantee”. Based on this project, the Primary Care Act 66/1972 and the Act on Specialized Medical Care 1062/1989 were supplemented with a Governmental Decree on Access to Care and Regional Cooperation (1019/2004). In addition to maximum waiting times, this Decree specified that the joint municipal boards of hospital districts have the responsibility for providing the specialized medical care prescribed in the Act in accordance with uniform medical principles and in collaboration with other hospital districts. The National Health Care Project was initiated in 2004 in order to secure access to treatment on equal grounds irrespective of the place of residence. In 2010, the MSAH published the uniform criteria on access to non-urgent care (MSAH, 2010). Other guidance for health care personnel has been available in the widely used Current Care Guidelines published by the Finnish Medical Society Duodecim.
Despite these measures, the geographical variation in medical practices persists in Finland (Keskimäki et al., 2014). This report showed that, for example, the rates for coronary revascularization and diagnostic tests are around two times higher in high activity areas than in low activity areas. The variations observed for caesarean sections and knee replacements were less pronounced. Over time these variations had increased for coronary procedures. In 2018 the MSAH initiated an updating of the uniform criteria, and the work is ongoing.
There has not been a systematic national level follow-up of medical practice variation until the recent reform plans established a new unit within THL to evaluate the performance of the new organizing entities, counties. Although the plans for reform have been deferred, THL will continue its analyses on care practices together with the MSAH.
Box5.4 assesses the integration of care. Box5.5 provides different methods used to obtain patients’ evaluation of care.
| Box5.4 | Box5.5 |
 |  |
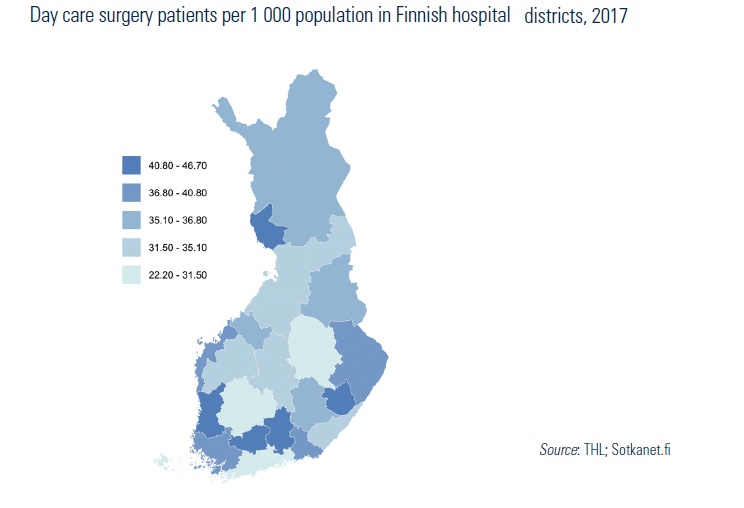
5.4.3. Day care
Finland had a somewhat slow start in developing day care in specialized health services due to the topographical remoteness of some areas. Nowadays, day surgery is more established and day care procedures currently account for slightly less than half of all surgical operations, although major variations between hospital districts exist (Fig5.3). Most hospitals and some larger health centres provide day care, mainly for minor surgeries, endoscopies and cardiac procedures.
Fig5.3