-
01 October 2019 | Country Update
Hospitals establishing patient advisory committees
2.9. Patient empowerment
The first patient advisory committee was established by the Kuressaare Hospital this summer. Tartu University Hospital (TUH) also established a patient advisory committee following this initiative. Both patient advisory committees are expected to advise the hospital management board on developing health care services, and help to bring patients and their caregivers perspective into a central role, which is an important step towards patient centredness. The new committees consist of patient representatives who have had previous personal experiences with the hospital. The committees act on an unsalaried basis.
Authors
2.9.1. Patient information
In 2008, a centrally managed e-health concept was introduced that aimed to make all health information available to patients and health professionals. The patient has the right to decide who can access his or her personal (not critical for life) information. The e-health system creates an information-exchange platform by establishing connections to the websites and databases of several actors. This should improve the continuity and integration of care by providing and exchanging the appropriate information about the patient for health care workers in different organizations. However, the e-health system is not explicitly designed to improve patient information.
Information related to health insurance is available from a variety of sources. The EHIF has set up websites, local service desks, telephone services and information leaflets, as well as regular mass media advertisements. Estonian citizens have access to personal information such as coverage, benefits received, reimbursed cost of health care services and medicine use through a state-managed central data exchange (“X-Road”), which uses ID cards and passwords for privacy protection. Furthermore, the EHIF website contains information on health service entitlements, prices, reports on health services and benefits utilization, as well as lists of contracted health service providers. The EHIF also publishes information about entitlements on receiving cross-border care in the EU.
The Ministry of Social Affairs and other state agencies (including the NIHD, the SAM and the Health Board) have designated websites and printed publications, mostly containing contact data, responsibilities and services provided, as well as reports and statistics of public interest. In addition, NIHD manages websites on health information (www.terviseinfo.ee) and other websites on prevention and promotion (e.g. www.alkoinfo.ee, www.hiv.ee, www.narko.ee and www.toitumine.ee). Health service providers have the legal responsibility to provide information on availability, accessibility and prices of services, which is done mostly through websites.
Public information on the performance and quality of the health system and health care provider is still limited. To bridge this gap, since 2012 the EHIF has reported on selected indicators of the Hospital Network Development Plan (HNDP) hospitals and in 2016 published a first report on quality indicators of selected medical specialties. In addition, the EHIF provides information on family physicians’ performance (see section 3.7.1 Paying for health services).
In addition to the national authorities, in recent years health care providers are increasingly sharing information (e.g. patient guidelines, replies to complaints) to patients on their websites.
2.9.2. Patient choice
The EHIF provides almost universal coverage and its coverage in terms of benefits is broad (see section 3.3.1 Coverage). As Estonia has a single-payer system, no competition or choice between different purchaser organizations exists. Since 2006, patients can choose the health care provider with the EHIF contract they prefer. Before then, choice was limited to the contracted providers of the EHIF regional department where a given patient was registered. At the primary health care level, all citizens in Estonia have to register on a practice list of the family physician of their choice. Family doctors may refuse an individual when the list is full or the person does not live within their catchment area. According to a survey, 96% of the population is aware that they can switch family physicians and 78% of patients are satisfied with the services of their family physician (Kantar EMOR, 2016). Furthermore, with a referral, a patient also has a free choice of specialist. However, this free choice may be constrained when there are waiting lists. Providers without a contract with the EHIF are freely accessible to everyone willing to make out-of-pocket (OOP) payments.
2.9.3. Patient rights
The basis for discussions and drafts of legislative documents on patient rights in Estonia is A Declaration on the Promotion of Patients’ Rights in Europe (WHO Regional Office for Europe, 1994). The draft of the Patient Rights Act was discussed in parliament in 1996 and 2002. In 2011, the topic was raised again by the parliamentary Social Affairs Committee, but these discussions have not resulted in any legislation. The rights and obligations of patients have been incorporated in the Law of Obligations Act (enforced in 2002). The Law of Obligations Act defines the contractual relationship between the patient and their doctor and requires the involvement of patients in decisions regarding their own health. Health care providers need written informed consent to be signed by patients before providing any health services. Doctors have a duty to inform patients about their health issues and required health services. The Act also states that a provider cannot promise that an operation will be successful or a patient will recover. The patient has the right to a second opinion paid for by the EHIF. Estonia has also signed and ratified the Biomedical Convention, which entered into force in 2002 and regulates, among other things, issues surrounding gene testing.
The EPAA counsels and represents patients who have complaints about such issues as malpractice, poor quality care and limited access to care. The EPAA processed 556 complaints in 2015 (EPAA, 2016). The vast majority of complaints are related to patient–provider contacts. A representative of the EPAA is also a member of the Health Care Quality Expert Commission, which assesses most complaints (see section 2.9.4 Complaints procedures).
The general level of patient rights protection remains rather weak. Yet the situation has been improving with increased awareness among patients about their rights.
Physical conditions and the construction of health facilities, including general building standards, are regulated by different legislative acts. Although standards are specified and all new buildings are required to ensure easy accessibility for all, including people with physical disabilities, in reality many older health facilities do not fully meet disabled people’s mobility needs.
2.9.4. Complaints procedures
The Health Services Organization Act and Law of Obligations Act jointly regulate the complaints procedures (mediation, claims) for health services and make the health care provider responsible for malpractice and low quality of health services. Most complaints are settled between the health care provider and patient, and there are no official data on how often this occurs. If damage to the patient’s health is suspected, or serious quality problems arise, official complaints are made to the Health Care Quality Expert Commission, which acts under the Ministry of Social Affairs. The Commission’s main role is to act as an independent counsellor for patients but its decisions have no legislative power. If the Commission finds the health care provider to be responsible for malpractice and causing health damage, the patient has a right to have their case heard in court and the Health Board could fine or withdraw the licence of the health care provider concerned.
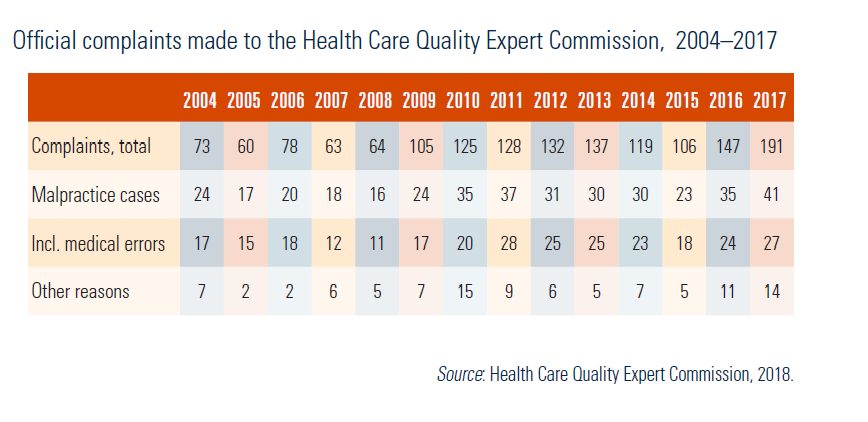
In 2017, the Health Care Quality Expert Commission managed 191 patient complaints (Table2.2), 41 (21%) related to malpractice, of which 27 (66%) were related to medical errors. Since 2004, the total number of complaints increased considerably, particularly in 2016 and 2017.
Table2.2
2.9.5. Public participation
The main mechanism for public participation has been the inclusion of representatives of insured groups in the EHIF 15-member Supervisory Board. Five members come from such organizations as the Estonian Union for Child Welfare, the Estonian Employees’ Unions’ Confederation, the Estonian Trade Union Confederation, the Estonian Association of Pensioners’ Societies and the Estonian Chamber of Disabled People. The EHIF Supervisory Board approves the EHIF’s long- and short-term strategies and yearly health insurance budget (see section 2.3 Organization). In addition, patients are represented in the Guideline Advisory Board, which was established in 2011 to improve the quality of health services by supervising the development of efficient and evidence-based clinical guidelines (see section 2.8.2 Regulation and governance of providers).
Since 1996, the EHIF (in collaboration with the Ministry of Social Affairs since 2005) has been conducting annual surveys on patient satisfaction with different aspects of the health system. The scope of the surveys has been broadened over time and now allows observing time trends. In general terms, the satisfaction of the population with health service access and quality has been relatively high over the years.
2.9.6. Patients and cross-border health care
The EHIF is responsible for all cross-border patient mobility issues. Insured individuals are entitled to receive EHIF covered services in the other EU Member States, Iceland, Liechtenstein, Norway and Switzerland. Directive 2011/24/EU on patients’ rights in cross-border health care sets out the conditions under which a patient on their own initiative may travel to another EU country to receive medical care and reimbursement. Furthermore, based on EC Regulation 883/2004, Estonian insured can use the European Health Insurance Card to receive health services abroad under equal conditions and equal tariffs as nationals of the Member State of treatment, including financial participation (cost sharing). The treatment is paid by the EHIF when on a temporary stay. The reimbursement does not cover travelling costs. Payments for health services provided in other Member States to persons insured with the EHIF increased almost three times during the period 2008–2011, from €1.4 million to €5.3 million and have since fluctuated around that level, being €5.4 million for 258 persons in 2016 (EHIF, 2017).
In addition, an Estonian insured may ask the EHIF for pre-authorization when planning to receive treatment abroad. This care cannot be denied if it is covered by the Estonian basic benefit package but cannot be provided in Estonia within a medically justifiable time-limit. Other national criteria applied in this decision are whether the service is medically justifiable, and if it is of proven medical efficacy, with a probability of success of at least 50%. EHIF payments for health services incurred abroad have increased from €1.4 million in 2008 to €3.7 million in 2016 (EHIF, 2017).
Information on the number of prior authorizations granted by the EHIF is available and is published in annual reports. The number of prior authorizations has increased from 18 patients in 2002 (EHIF, 2003) to 244 patients in 2016 (EHIF, 2017). In 2015, 64 persons were referred for treatment abroad, 141 for examinations, and 39 to search for unrelated bone marrow donors through the Finnish Red Cross. The majority of patients were treated in Finland and Sweden, while the number of examinations was highest in Germany and Finland (EHIF, 2017).
As for patients coming from abroad to receive treatment in Estonia, the spa hotels are active in attracting foreign customers. Also, dental care, plastic surgery, ophthalmology, in vitro fertilization treatment, radiology and some other diagnostics services are among services provided to cross-border patients. Most clients come from neighbouring countries, such as Finland and Sweden, but increasingly also from the Russian Federation and Latvia (Aaviksoo et al., 2010).