-
30 January 2022 | Country Update
The salary growth of health care workers in 2021 was accelerated by the overtime work and bonuses related to the COVID-19 crisis -
11 February 2021 | Country Update
Increased funding for nurses and medical supporting staff in primary healthcare centers -
23 November 2020 | Policy Analysis
New payment model for stroke treatment -
23 October 2020 | Country Update
Changes in financing Personal Protective Equipment -
14 July 2020 | Country Update
Increased distance allowances for family physicians operating in rural areas -
03 December 2019 | Country Update
World Bank assessment of new payment model for rural hospital -
29 January 2019 | Country Update
Health workers’ collective agreement for the next two years agreed
3.7. Payment mechanisms
In 2021 the Estonian Health Insurance Fund (EHIF) started to pay for the additional staff for the primary care providers working under contracts of primary healthcare centers. With this change, a primary care provider can hire an additional nurse or other medical supporting staff (e.g., a mental health nurse or clinical psychologist) to the team in addition to the minimum of 3 family doctors and 3 family nurses. Previously, every family physician could also hire a second nurse. The maximum EHIF compensation covers the cost of 6 nurses and one additional nurse or other medical specialist per 3 family physicians. The aim of the change is to tailor the service provision according to the actual needs of the patient lists. The providers can choose which expertise is needed the most. Furthermore, it is also possible to get compensated based on the actual working hours, making the system even more flexible and not assuming full time employment. A monthly allowance is paid to providers who applied for the additional funding. It is estimated that the change will result in a budget increase of 1,9 million euros.
In total there are 40 primary healthcare centers contracted with EHIF, including 225 family doctors with patient lists.Primary healthcare centers cover almost 30% of total patients in the country.
Authors
The Estonian Health Insurance Fund (EHIF) has launched a Stroke Patient Pathway Pilot which aims to improve patients' quality of life through developing a more integrated care pathway from the patient's point of view. The purpose of the change in payment system is to improve health outcomes, motivate cooperation and coordination, and to give medical institutions opportunities to direct additional resources to stroke treatment.
During the pilot from 1 July 2020 to 30 June 2021, EHIF will test a bundled payment for the first time. The bundled payment is calculated for the entire patient pathway of a patient with ischemic stroke. For quality and outcome measurement, the International Consortium for Health Outcomes Measurement (ICHOM) standard set of indicators for stroke will be used, including Patient-Reported Outcomes Measurement Information Systems (PROMIS) Global-10 for patient reported outcomes.
The bundled payment aims to cover the whole course of treatment for insured patients, consisting of the following components: (a) the cost of treating ischemic stroke; (b) the cost of treating the complications. The agreed length of the pathway is 365 days (or until death or recurrent stroke). Although the coordination and continuity of the treatment must be ensured between the different levels of the health care system and between the health care system and the social system, the payment only covers acute treatment, rehabilitation, follow-up and nursing care. Primary care and social services are not included. In order to ensure outpatient rehabilitation close to home, institutions providing active treatment for stroke can order services from family physicians with no cap (the therapeutic services like physiotherapy, speech therapy and psychologist services are in other cases capped with 3% of total capitation). The bundled payment was calculated using historical data, with the rehabilitation payments added to the bundled payment as it was agreed that the provision would otherwise be insufficient. As a statistical analysis showed that depending on the initial treatment (thrombectomy, thrombolysis, other treatment) and the age of the patient, the bundled price differs, so the EHIF formed 7 treatment routes at different prices.
Participating providers were identified through a two-stage application round. For eligibility, the projects had to find solutions for 6 development needs (e.g., create a coordinating role, implement a single care plan etc.) which were identified together with stakeholders. In total four hospitals were selected as partners.
All hospitals providing services will be paid according to the current system (fee-for-service, DRG). At the end of the pathway, a comparison will be made on every treatment case between the amount paid and the calculated bundle payment for the whole patient pathway. The difference on every case will be summarized. If the amount paid is less than the expected cost of the bundled payment, the EHIF pays the difference in the cost to the hospital in charge of the pathway. Otherwise, the service provider will pay the difference to the EHIF. An exemption is made for cases more costly than 100,000 euros. It is expected that the changes in the payment model will result in a budget increase of 520,000 euros over a 6-month period in 2020.
The change in payment model and the measurement of patient characteristics, outcome and process indicators will be applied to all stroke pathways in the four hospitals starting in the period from 1 July 2020 to 30 June 2021. A conclusion about the effectiveness of the pilot will be made by 30 June 2022. In the piloting phase, the outcomes are not tied to payments, but the EHIF has announced that this will be the case if the model proves its effectiveness and becomes applied as a standard practice.
Authors
Starting from September 2020, EHIF adopted a new model to finance personal protective equipment (PPE) for healthcare providers. Before the COVID-19 pandemic, EHIF financed PPEs through service prices, calculating the average need per service and incorporating the cost into the total service price.
The renewed financing scheme aims at providing additional flexibility to increase PPE funding when the higher need occurs. The amendment allows for the reimbursement of additional costs for PPEs and disinfectants incurred during the spread of a novel particularly dangerous infectious disease (defined in the Communicable Diseases Prevention and Control Act). The only PPE costs covered are those that are not reimbursed through service prices.
The changes are based on the financial measures implemented in spring 2020 following the declaration of the emergency due to the spread of COVID-19. EHIF has calculated the maximum cost of PPEs and disinfectants for the service providers considering the volume of services provided. The calculated amount is fully reimbursed if the medical institution can prove documented proof about the purchase of PPEs and disinfectants at least to the calculated amount. The period of purchasing PPEs is limited to 30 days before and including the emergency or preparedness period announced by the Health Board in accordance with the Health Insurance Act. If the additional cost of the service provider during this period is lower than the calculated amount, a coefficient is applied to the reimbursement of the cost in order to bring the reimbursable amount in accordance with the invoices of purchased PPE and disinfectants.
EHIF has assessed that this change may cost up to 16 million euros per year, but also has stated that it only occurs when the need arises as announced by the Health Board. The Government will determine the funding of these costs during an emergency period.
Authors
References
Since April, the distance allowances for all family physicians operating outside the major centers were multiplied. Until March 2020, family physicians operating in rural areas which were located 20-40 km from the nearest hospital received an additional allowance of EUR 196.55 per month, which increased to EUR 823.41 in April. This allowance will be paid to all providers operating outside of Tallinn and Tartu (Estonia’s two biggest cities) and to family physicians working in adjacent municipalities. After the amendment, when a family physician operates in a location which is more than 40 km from the nearest hospital, they receive a monthly allowance of EUR 1646.82, increased from EUR 563.15. The higher allowance is also paid to family physicians operating on an island.
As a result of the changes, 400 family physicians will receive additional distance pay, which previously affected 179 family physicians. The purpose of paying the distance allowance is to ensure the availability of primary medical care outside larger centers by motivating family physicians to work in rural areas.
Authors
In April 2018, the Estonian Health Insurance Fund (EHIF) introduced a global budget as the main payment mechanism to fund a rural hospital on the island of Hiiumaa (see log on “The Estonian Health Insurance Fund is piloting a global budget based payment model for one hospital“ from April 2018 for an overview). In 2019, the World Bank conducted an assessment of the pilot and primarily focused on the design of the new payment mechanism.
The analysis highlighted that Hiiumaa hospital’s contract will require a revision of the performance indicators in order to expand the current focus on utilization to include accountability for access, quality, safety, and patient experience. Furthermore, the analysis concluded that the limited evidence on the impact of the new global budget models in other countries and the other ongoing payment reforms in Estonia do not support the expansion of the global budgets pilot to other hospital in the short term. The recommendation is to first further refine and strengthen the piloted payment system.
Representatives from provider associations and health professionals’ unions signed the collective agreement for the next two years in November 2018. The minimum hourly wages for doctors, nurses and other health care professionals will increase up to 13.30 euros, 8.00 euros and 5.00 euros respectively by 2020. This translates into an increased minimum wage of 18.1% for doctors, 16.8% for nurses and 19% for other health professionals. In addition, night and weekend shift allowances, compared to the minimum required by the law, will be gradually introduced. These negotiations received relatively little public attention compared to previous negotiations. This is partly due to the promising economic environment which enabled the representatives to opt for an accommodating approach in the pre-election period.
Collective agreement (in Estonian) available at Source: https://arstideliit.ee/wp-content/uploads/2018/11/Tervishoiuvaldkonna_kollektiivleping_30.11.2018.pdf
Authors
3.7.1. Paying for health services
The actual payment methods, service prices and benefits package are all included and regulated in a single government-approved health service list. The management of this list is the responsibility of the EHIF but the government gives its final approval. All providers are paid the same prices and there is no adjustment for hospital characteristics, such as teaching status. Since 2002, the EHIF’s health service list is approved by the government in order to increase public accountability and to make it less vulnerable to provider influence, as it had been when the Minister of Social Affairs was solely responsible for amendments and updates. The list of services and prices is updated at least once a year. The price list contains more than 2000 different items, including a whole range of different payment methods. Please refer to Table3.8 for an overview of the most commonly used payment methods, which will be further discussed below.
Table3.8
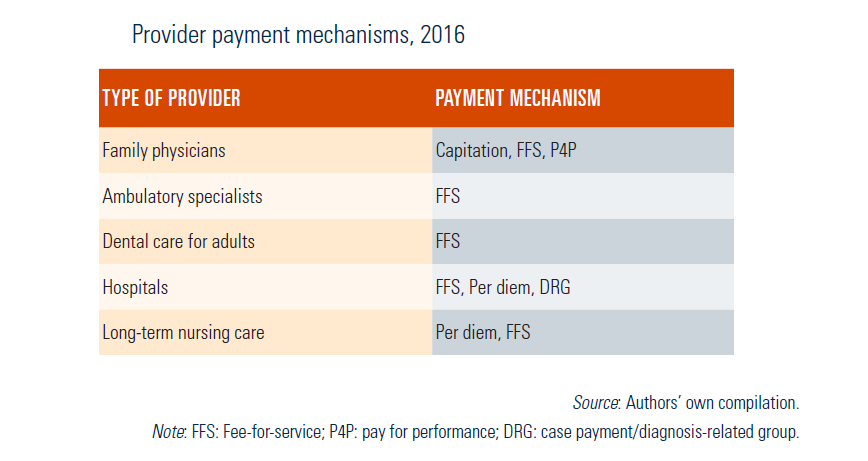
The payment system for family doctors has been redesigned since the early 2000s, to provide them with incentives to take more responsibility for diagnostic services and treatment, to provide continuity of care and to compensate them for the financial risks of caring for older people and working in remote areas. In primary care, family doctors and nurses contracted by the EHIF are paid via a combination of capitation, basic allowances, fee-for-service and a quality bonus system. There are three funds used for fee-for-service. These include the investigation fund (for different laboratory tests), the therapeutic fund (e.g. physiotherapy and speech therapy) and the activity fund (minor surgical procedures) (see Fig3.7). Together, these payments make up the total budget for each practice. Practices receive monthly prepayments for capitation, allowances and fees, which are recalculated four times a year to reflect changes in the patient list (as patients can change family physicians). The average size of the family doctors’ list is about 1600 persons, but the average income of practice varies widely according to the structure of the people on the list and the different allowances the family doctors can apply for. In 2016 the average monthly practice income was about €10 700.
Fig3.7
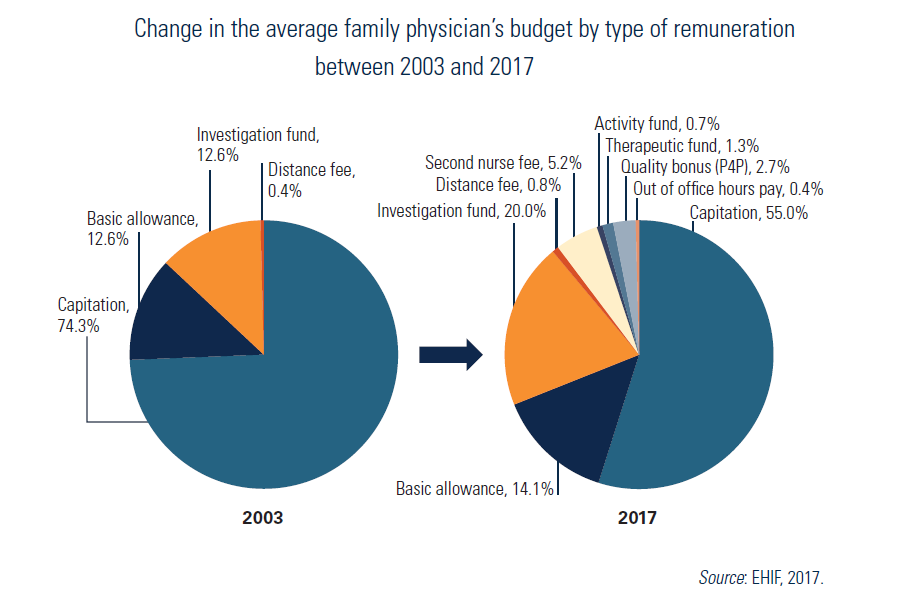
After the family physician payment reform of 1998, the capitation payment was similar for all people, irrespective of their age. Age-adjustment was introduced after only one year, forming three capitation groups: up to 2 years of age, 2–70 years of age, and older than 70 years. In 2012, five new capitation groups were agreed: patients aged up to 3 years, 3–6 years, 7–49 years, 50–69 years and over 70 years.
Practices also receive a basic monthly allowance to cover costs of the premises and transport for doctors or nurses. Additional and more marginal payments are made to compensate family physicians in remote areas. Furthermore, a family doctor’s income depends not only on practice list size but also on performance, so that any money spent on unnecessary analyses and procedures will reduce payments. In the collective agreement negotiations in 2013, an additional allowance for family doctors employing a second nurse was agreed. The aim of this additional allowance was to support the nurse’s increasing role in monitoring patients with chronic diseases and acute health disorders as well as in counselling and prevention. A family doctor has to fulfil certain criteria to receive this additional remuneration, for example separate visiting hours for the second nurse and room requirements. Starting from 2014, family physicians may also receive an allowance for overtime work, and nurse(s) for appointments outside of working hours (before 8:00 or after 18:00).
From 2016, the EHIF has increased the share of the basic allowance and reduced the share of capitation in the payment scheme. Furthermore, in 2017 a new basic allowance has been introduced for primary health care centres that should motivate individual primary health care providers to form groups and provide a wider scope of services. The primary health care centre basic allowance includes additional funds for management, information technology (IT) developments and more spacious rooms. The primary health care centres are eligible for this allowance when at least three family doctors with at least 4500 individuals on their list work together in one location; they also provide physiotherapy and midwife services (providing home nursing will be compulsory starting from mid-2018) and have extended opening hours (from the compulsory 8 hours to 10 hours per day).
Family physicians can receive separate additional fee-for-service payments up to a maximum of 41% of their total capitation payment if they perform well according to the quality bonus system standards. The maximum fee-for-service payment rate for family physicians who do not attain the quality goals is 39%. These differentiated rates are used to provide incentives for family physicians not only to participate but also to achieve good results and to promote improvements in quality of care.
The new quality bonus system was introduced in 2006. The main purpose of this initiative was to increase the quality and effectiveness of preventive services, as well as to improve monitoring of chronic diseases. The quality bonus system highlights the importance of clinical guidelines and performance monitoring at primary health care level. It is the only quality rewarding system that has ever existed in Estonian health care. The cost of the scheme, about 2% of the primary health care budget, is relatively small and there is ongoing discussion to expand the quality bonus system and make it more attractive. The quality bonus system includes three domains: disease prevention, chronic disease management and additional activities. The quality bonus system is a joint initiative of the EHIF and the Estonian Family Physicians Association. A key factor in implementing the quality bonus system has been the electronic billing data collection system, which enables monitoring of family physicians’ activities without the need for additional data collection. Since its introduction, the number of participating family physicians has risen from 50% in 2006 to 97% in 2014, reflecting its broad acceptance. Despite its small financial contribution, the quality bonus system has strengthened disease management for patients with hypertension or diabetes or after acute myocardial infarction (Fig3.8), and nearly all the indicators of disease management have improved. However, three of the four indicators of prevention have not yet improved (see also 7.4.2 Health service outcomes and quality of care).
Fig3.8

Since 2015 the participation in the quality bonus system has been obligatory for all family doctors and the individual results are publicly reported. In 2015 the World Bank conducted a study on Health Care Integration in Estonia. In response to the results of the study, in 2016 the EHIF made considerable changes to the quality bonus system and raised the payment by 25% (compared to 2015). The focus of the quality bonus system has been shifted from rewarding family doctors for single activities to bundled activities. Indeed, the scheme now rewards coordinating the provision of a full set of recommended services rather than single procedures or services, i.e. administering all necessary vaccinations for children up to 3 years old rather than doing a single vaccination. In addition, indicators for the correct prescription of medication for the chronically ill have been added to the quality bonus system indicators. With the help of e-prescription data, the EHIF can measure whether the family doctor has prescribed the medications in accordance with clinical guidelines, i.e. oral hypoglycemic (metformin) for patients with diabetes. In 2016 a separate payment was introduced in the quality bonus system for accredited providers. The accreditation process is led by the Estonian Family Physicians Association.
In 2013, the EHIF started remunerating new innovative e-consultations, in which family physicians consult with specialists through the health information system without sending the patient to the specialist care provider. The e-consultation should support family doctors in assuming more responsibility for patient care and should improve cooperation with specialists. Moreover, this is expected to lower the demand for specialist care, shorten the care episode and provide relief for long waiting times for some specialties. The e-consultation has to follow a standardized format (by specialty), which should better enable specialists to give adequate advice. During 2016, 603 family doctors had 5597 e-consultations with seven different HNDP hospitals (EHIF, 2017). This still accounts for only a very small share of total ambulatory specialist care visits.
Specialist care is mainly remunerated through fee-for-service payments, per diems and diagnosis-related group (DRG)-based payment methods. The main method in outpatient care (laboratory tests, radiology, etc.) is fee-for-service payment, whereas for day surgery and inpatient care, a mix of fee-for-service, per diems and DRG-related payment methods is used. Day surgery and inpatient fee-for-service payment involves also per diem-based units. The per diem should cover the costs of basic examination, diagnosis and treatment planning, nursing, meals, simple medical procedures, laboratory tests and pharmaceuticals.
The EHIF implemented a DRG-based payment system for inpatient services in 2004. The DRG system was mainly seen as a tool to increase efficiency. Another motivation for introducing DRGs was that the old fee-for-service and per diem payment systems had led to volume inflation. In 2001, the EHIF began work on adapting the Nordic DRG system (NordDRG) by identifying areas of variation in activity between Estonian and Scandinavian hospitals, calculating prices for reimbursement in Estonia and providing hospitals with feedback on their activity by NordDRG group. The large amount of detailed diagnostic data available to the EHIF through the invoicing system facilitated this process. By 2003, all primary classifications were implemented, and from 2004 the NordDRG system became operational. The NordDRG system is used in combination with other payment methods already in place, so the price of a case will be calculated based on the price list and NordDRGs and reimbursed proportionally. To minimize any financial risk, the proportion of DRG payment for each case was gradually raised from 10% in 2004 to 70% in 2009 (EHIF, 2009). All inpatient care cases, as well as outpatient care cases involving surgical procedures, fall under DRGs. However, some types of care, such as psychiatric, rehabilitation and follow-up care, are not reimbursed through DRGs. There are also some exemptions according to the principal diagnosis (e.g. chemotherapy), services provided (e.g. organ transplantations) and referred cases. In addition, cases that are too low or high in cost are reimbursed through fee-for-service.
In principle, health service prices should cover all costs related to providing services except those related to research and teaching activities, which are funded separately. All prices approved are maximum prices, and providers and the EHIF can agree on lower prices in the contracts. Revision of service prices and payment methods can be initiated by provider or specialist associations or by the EHIF (see also section 3.3.1 Coverage).
From July 2003, capital costs have been included in the prices paid to providers by the EHIF in order to ensure geographical consistency and fairness in infrastructure development. The mark-up has been calculated according to providers’ optimal capacity per bed (based on an optimal number of square metres per bed). Capital cost funds are now allocated on the basis of activity, and there is no clear link to capital investment needs. However, some of the health care providers receive ERDF infrastructure investments, which may increase disparities among the different providers (see also section 3.6.2 External sources of funds).
3.7.2. Paying health care personnel
During the Soviet era, health care professionals were, similar to civil servants, working as salaried employees in health facilities owned by the state or municipalities. Salary levels were determined centrally. Since the early 1990s, new health care legislation allowed individual providers to work according to private law for the first time and gave institutional providers more autonomy under a different legal status. Although many institutions are still controlled by the state or municipalities, the level of salaries is now established through individual negotiations between employers and employees, taking into account the collective agreements between associations.
Health care professionals’ salaries are determined by the minimum amount of cases contracted with a provider by the EHIF. On average, salaries account for approximately 60% of total hospital costs. All health care professionals and providers now hold individual contracts with hospitals or health centres, although these are sometimes based on general salary agreements for specific groups. The Estonian Medical Association and the Estonian Nurses Union negotiate the levels of minimum hourly wage/salary for their respective professions with the Estonian Hospital Association. The Ministry of Social Affairs and the EHIF are also involved in these negotiations. In 2012 negotiations got stuck and resulted in a 25-day strike of health care workers. The wage negotiations for the 2015–2016 period were particularly lengthy and difficult and resulted in pay rises above the average wage growth in the country. The wage negotiations have put great pressure on the EHIF budget and necessitated difficult trade-offs between higher prices and service volume cuts. After difficult negotiations for more than 6 months between representative bodies of health professionals and medical associations, and unions a collective agreement was finally reached in April 2017, which will last until April 2019.
The minimum hourly wages for doctors, nurses and other health care professionals increased up to €11.35, €6.85 and €4.20 respectively by 2018. This translates into a biannual increase of minimum wages by 13.5% for doctors, 24.5% for nurses and 27.3% for other health professionals. The 2017–2018 negotiation process stands out because of its length and scope, applying a broader health system focus instead of merely aiming at wages and working conditions. Health professionals pressured the government to find a solution securing the long-term sustainability of health insurance financing (see section 6.1 Analysis of recent reforms).
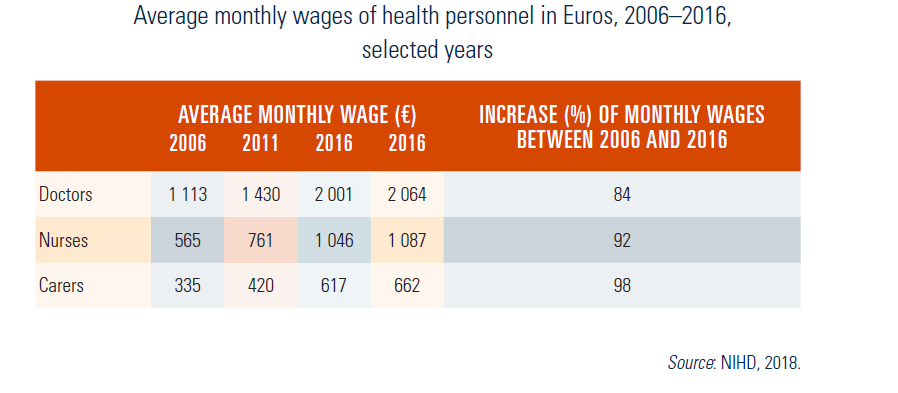
Although health care providers are private entities, the NIHD monitors their financial status and overall salary levels through statistics and annual salary surveys (Table3.9).
Table3.9