-
14 January 2022 | Policy Analysis
The new national health system (GeYS) has introduced different financing arrangements that reduce out-of-pocket spending -
30 September 2014 | Country Update
Beneficiaries and co-payments
3.4. Out of pocket payments
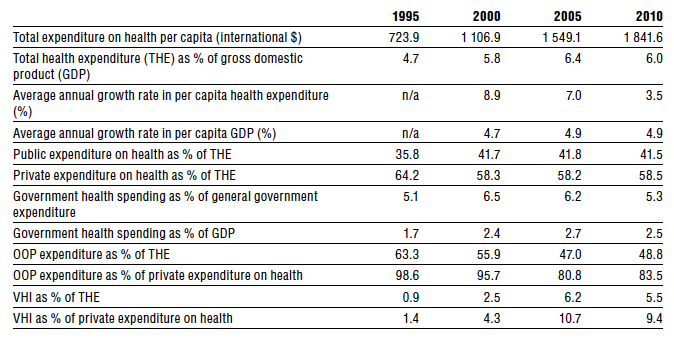
OOP payments represent over 83% of private health care expenditure, or nearly half of THE. Although OOP spending as a share of total private expenditure has declined since the 1990s, it remains at a very high level relative to other EU countries. During the same period, private health insurance rose considerably as a share of private expenditure, from 1.4% in 1995 to 9.4% in 2009 (Table3.1).
Table3.1
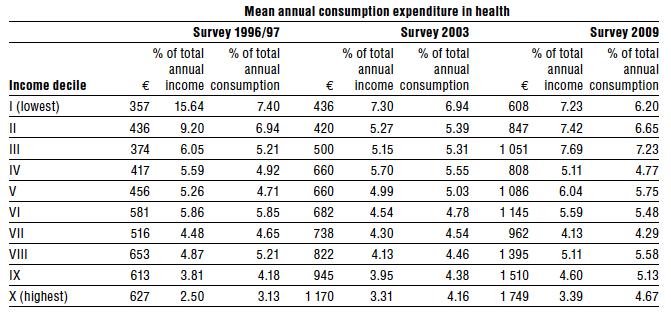
Household surveys conducted every six years by the Department of Statistics and Research in the MoF are an important source of data on OOP expenditures (Family Budget Surveys, 1999, 2006, 2011). According to these data the mean annual OOP expenditure for health services per adult equivalent [4] in the lowest income decile was €357 in 1996/97, €436 in 2003 and €608 in 2009. Among those in the highest income decile, the corresponding figures are €627, €1170 and €1749, respectively (Table3.2). Low-consumption and low-income households spend a higher proportion of their annual income and consumption on health compared to richer households, which reveals that the distribution of health expenditure is regressive.
Table 3.2
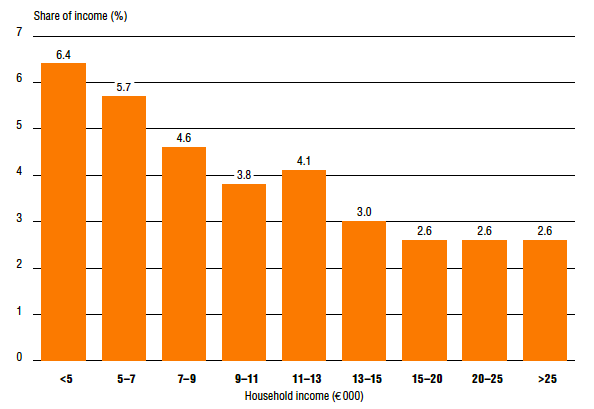
The findings of a household survey from 2002 by the Harvard School of Public Health are similar (Hsiao & Jakab, 2003). The median household, reporting an annual income between £C9000 (€15 457) and £C11 000 (€18 892), was found to spend nearly 4% of its income on health care services. Those with an annual household income below the median level spent 4.6 – 6.4% of their income on health, while those above the median income level spent 2.6 – 3.0% of their household income on health (Fig3.6). Expenditure levels for households that spend a large share of their income on health are increasing steadily, indicating that households with chronic or severe acute illness may face catastrophic levels of health expenditure. The financial burden of health expenditures has increased more for lower income households than for those with a higher income.
Fig3.6
The burden of OOP payments, especially for low- and middle-income households, is quite large. One possible explanation for such high OOP expenditures is that for reasons including long waiting lists, quality issues and health illiteracy, most people choose to purchase health care services from the private sector even though they are entitled to free access in the public sector.
- 4.The OECD scale counts the head of the household as 1.0 unit, additional adults (aged over 13) as 0.5 units and children (13 years of age and under) as 0.3 units. For example, a household of four of which two are aged 40 and 30 and the other two are aged 12 and 6 have an equivalent household size of 1+0.5+0.3+0.3=2.1. ↰
The new national health system (GeSY) has introduced a number of new methods of financing. There has been a shift from a predominantly tax-funded system that financed public sector health services together with high direct private payments from citizens to the private sector to a system of proportional contributions from beneficiaries based on their income and with a concomitant matching contribution from the government for each beneficiary. This adopts a more progressive approach to financing and coverage that includes all levels and strata of society such as dependents of beneficiaries, the unemployed and other low-income and socially disadvantaged persons.
Income contributions in the new scheme are as follows:
- employees, pensioners, government officials and income earners: 2.65% of gross income;
- employers for each employee: 2.90%;
- self-employed: 4.00%; and
- state/government for each employee, self-employed, government officials and pensioners: 4.70%.
All of the above groups are required to pay contributions levied on their gross income if they have any income. The maximum amount of gross annual income on which contributions are paid is €180 000.
The funds collected form the Health Insurance Fund, which is administered by the Health Insurance Organisation (HIO). The HIO is a public, independent organisation whose role is to manage the Fund, ensure access to and provision of health services to beneficiaries without adverse discrimination, and to contract with health care providers.
In addition to the Health Insurance Fund, there are combined cost-sharing arrangements comprised of low co-payments and personal contributions with annual caps; these aim to create a net of high financial protection without creating serious financial barriers to access by contributing to reduce unnecessary use of health services. So far, out-of-pocket payments, which were the third highest in the EU under the old system, have declined by 68%, from 2018 to 2020.
Examples of user charges are copayments of €15 if the maximum number of annual visits to the personal doctor/paediatrician is exceeded, co-payments of €6 for outpatient specialist visits with referral from a personal doctor/paediatrician, and €25 personal contributions without referral, which is accompanied with a €150 per year cap reduced to €75 for certain vulnerable groups such as guaranteed minimum income recipients and low-income pensioners.
References
• Abolition of class B beneficiaries
• New criteria for the acquisition of the medical card
• Introduction of co-payments for beneficiaries as follow:
€10 for a visit to the Accident/Emergency Departments,
€3 for a visit to a GP,
€6 for a visit to a specialist and
€0.50 for each prescribed pharmaceutical product and laboratory test with a maximum charge of €10 per prescription.
Exceptions apply for certain vulnerable groups.
3.4.1. User charges
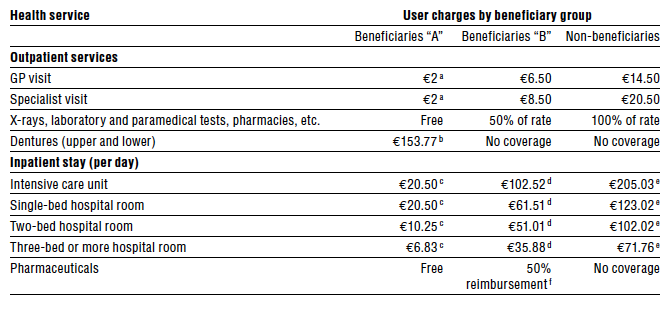
Approximately 85% of the population has free or reduced rate access to public health care services; the rest of the population pays full rates set by the Ministry of Health. However, for those patients in beneficiary group “B” and non-beneficiaries who use the public sector for their health needs, user charges can be substantial (Table3.3). Data from the Ministry of Health show that the majority of non-beneficiaries choose the private sector for health care, as only a small amount of public revenues were raised in 2009 from payments by non-beneficiaries, amounting to barely 1.8% of total hospital expenditures (€6 million).
Table3.3
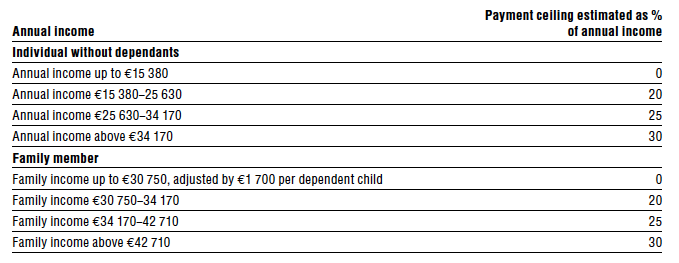
An interesting element of the fee schedule is the payment ceiling for hospital care, estimated as a percentage of annual income for every beneficiary, based on income level and the number of dependants. Expenditures beyond this ceiling must be paid out of the hospital budget. For example, the payment ceiling for a two-member family with €40 000 annual income is €2141. Table3.4 shows the income ranges, and the corresponding maximum percentage of annual income that can be spent on hospital care. This provision protects individuals from catastrophic levels of expenditure on inpatient care.
Table3.4
The cabinet, followed by the parliament, is responsible for approving user charges policies, setting prices and imposing user charges, based on proposals made by the Ministry of Health.
3.4.2. Direct payments
Theoretically, most medical services are covered and should be provided by the public sector to all beneficiaries in group “A”, except for some dental services such as orthodontics, fixed prosthetics and implants. For those services, patients must visit private dentists and pay out of pocket. In very few instances when for various reasons the public sector cannot provide a particular service, services can be purchased from the private sector. Direct payments are a common means of provider reimbursement for semi-state organizations and workers’ funds, as well as for many VHI schemes.
3.4.3. Informal payments
There is limited anecdotal evidence of informal payments in the public and private sectors. High physician salaries and very strict legislation generally prevent informal payments, although in some cases it may occur. For example, women who want to deliver their child in a public hospital with the gynaecologist or obstetrician of their choice usually offer a gift to their doctor.