-
31 March 2025 | Country Update
National Health Insurance Fund budget grows by 16% in 2025 -
15 March 2021 | Policy Analysis
National Health Insurance Fund budget for 2021 foresees a 13% increase -
09 March 2020 | Policy Analysis
National Health Insurance Fund budget for 2020
3.1. Health expenditure
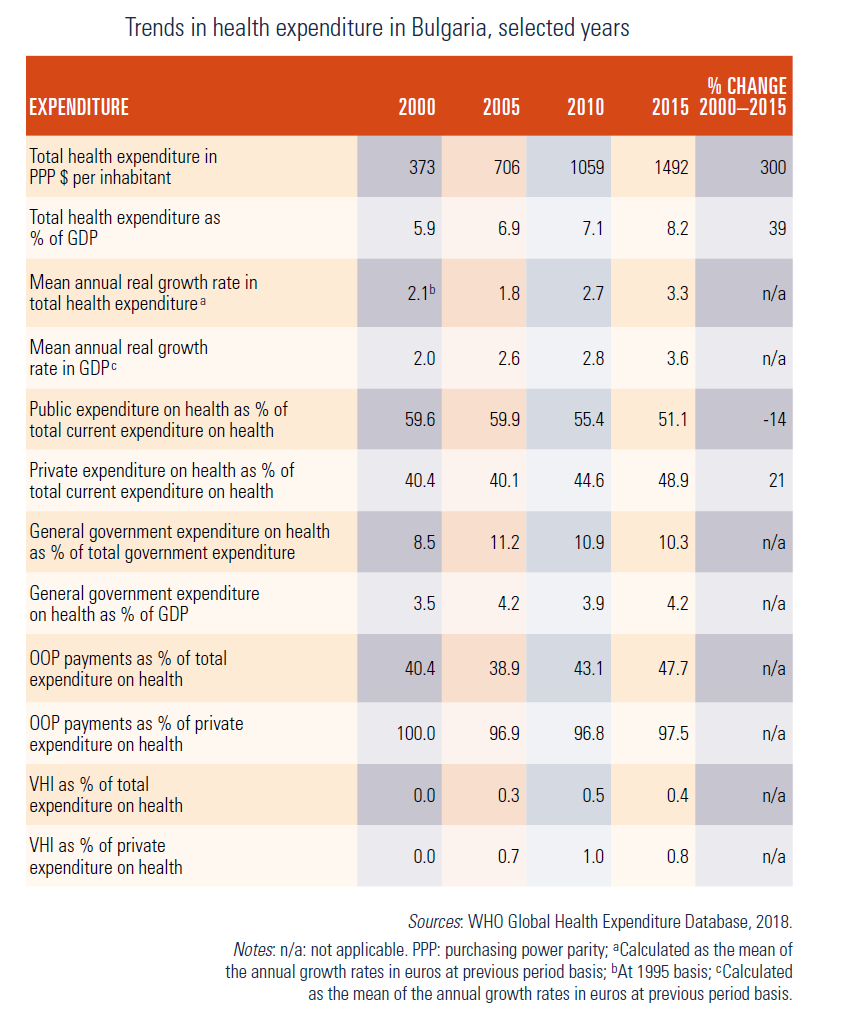
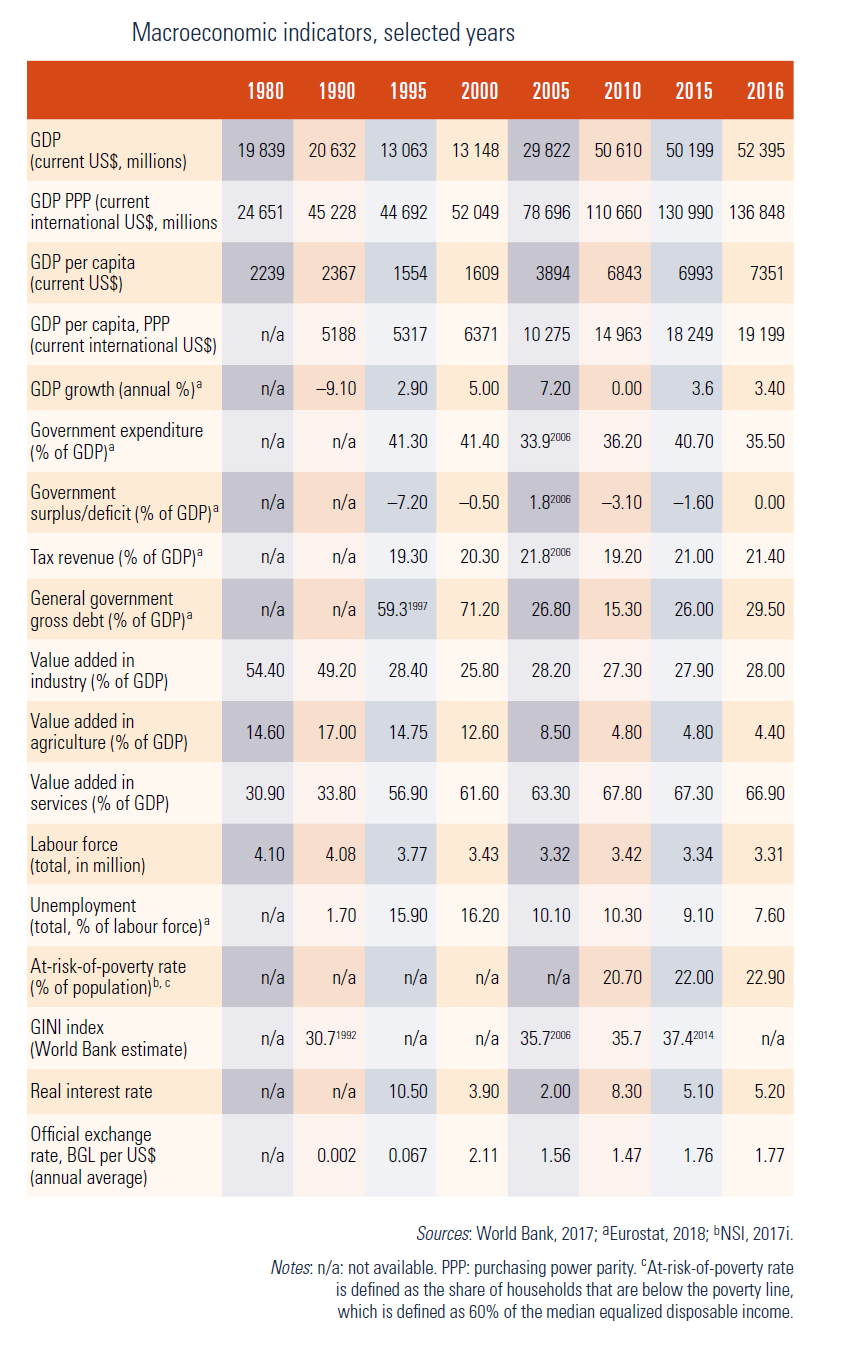
Bulgaria has a mixed public–private health care financing system. Health care is financed from compulsory SHI contributions, taxes, OOP payments, VHI premiums, corporate payments, donations and external funding. Since the introduction of an SHI system in 1998–1999, the total health expenditure in absolute value and per capita has constantly increased even during the financial crisis in 2008–2009. The total health expenditure as a share of GDP equally increased (see Table3.1).
Table3.1
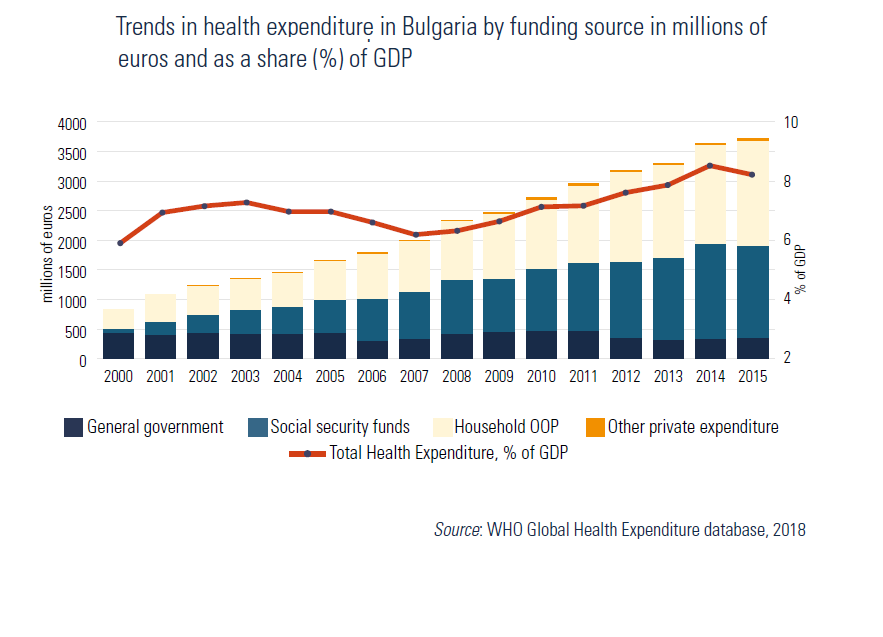
Bulgaria’s total health expenditure as a percentage of GDP is below the EU15 average (Fig3.1). Total health expenditure as a percentage of GDP increased from 4.7% in 1998 to 7.2% in 2001 (WHO Regional Office for Europe, 2018). In the following years, it decreased slightly to 6.5% in 2007, and increased to 8.2% in 2015 (Eurostat, 2018), surpassing all new EU Member States (except Slovenia) and the average for the EU13 average (Fig3.2). With a shrinking GDP base in 2009 due to the financial crisis, health expenditure increased compared with the previous 3 years and reached 7.1% in 2009. Thus, total health expenditure increased steadily in absolute value as well (Fig3.3). The slight decrease in total health expenditure as a share of GDP between 2010 and 2011 (Fig3.2) might be a reflection of the GDP increase surpassing the growth of health expenditure in 2011.
| Fig3.1 | Fig3.2 |
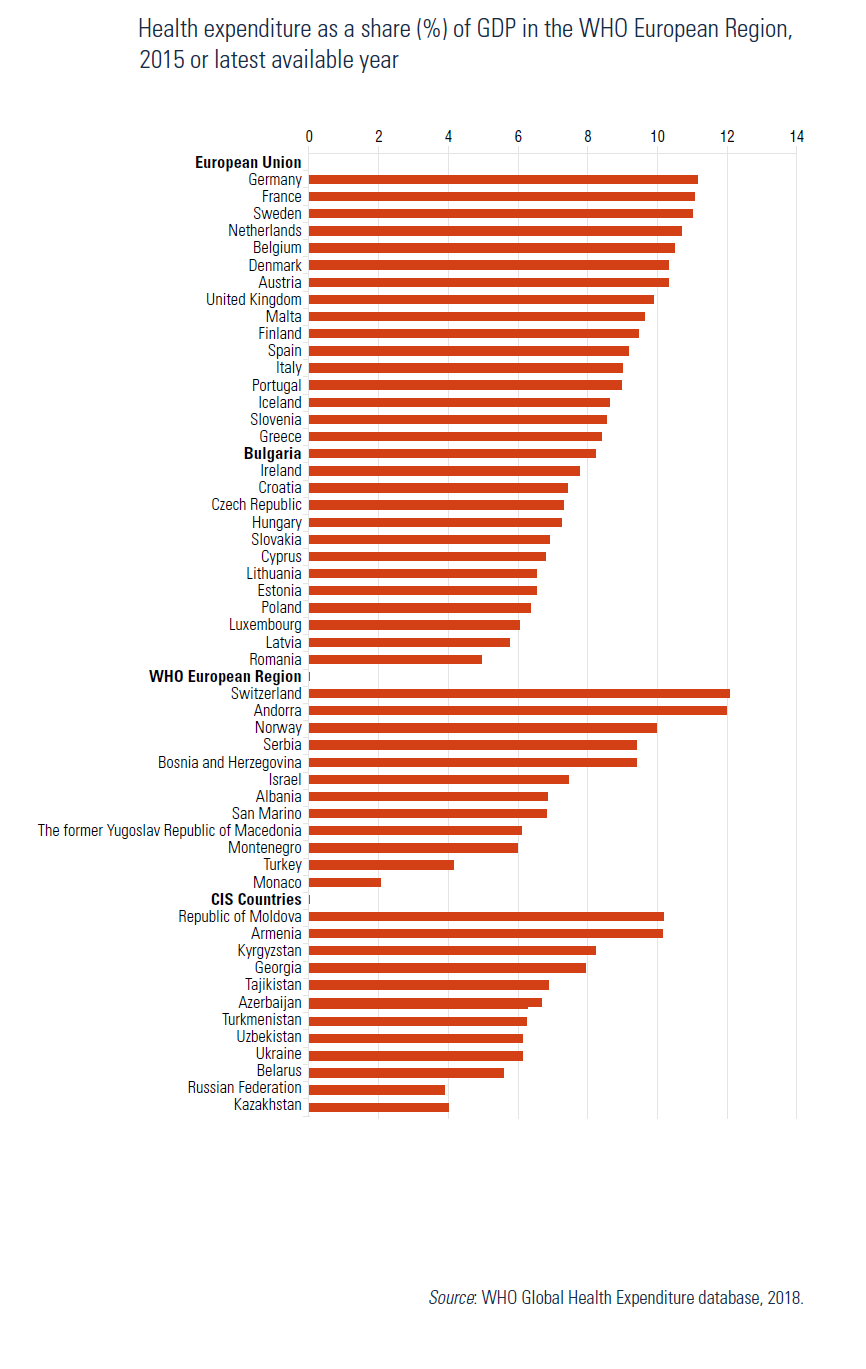 | 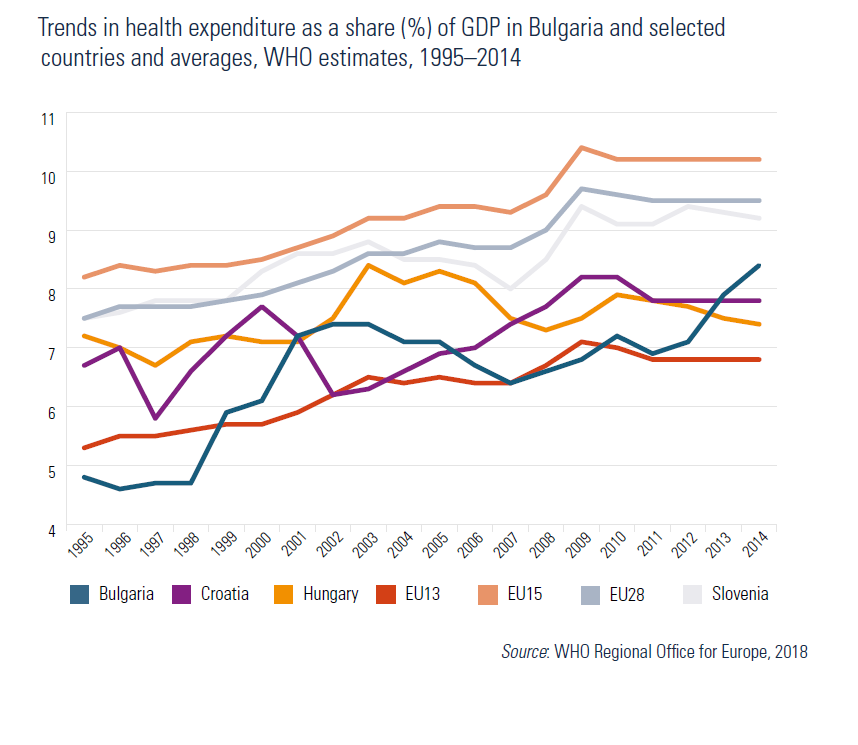 |
Fig3.3
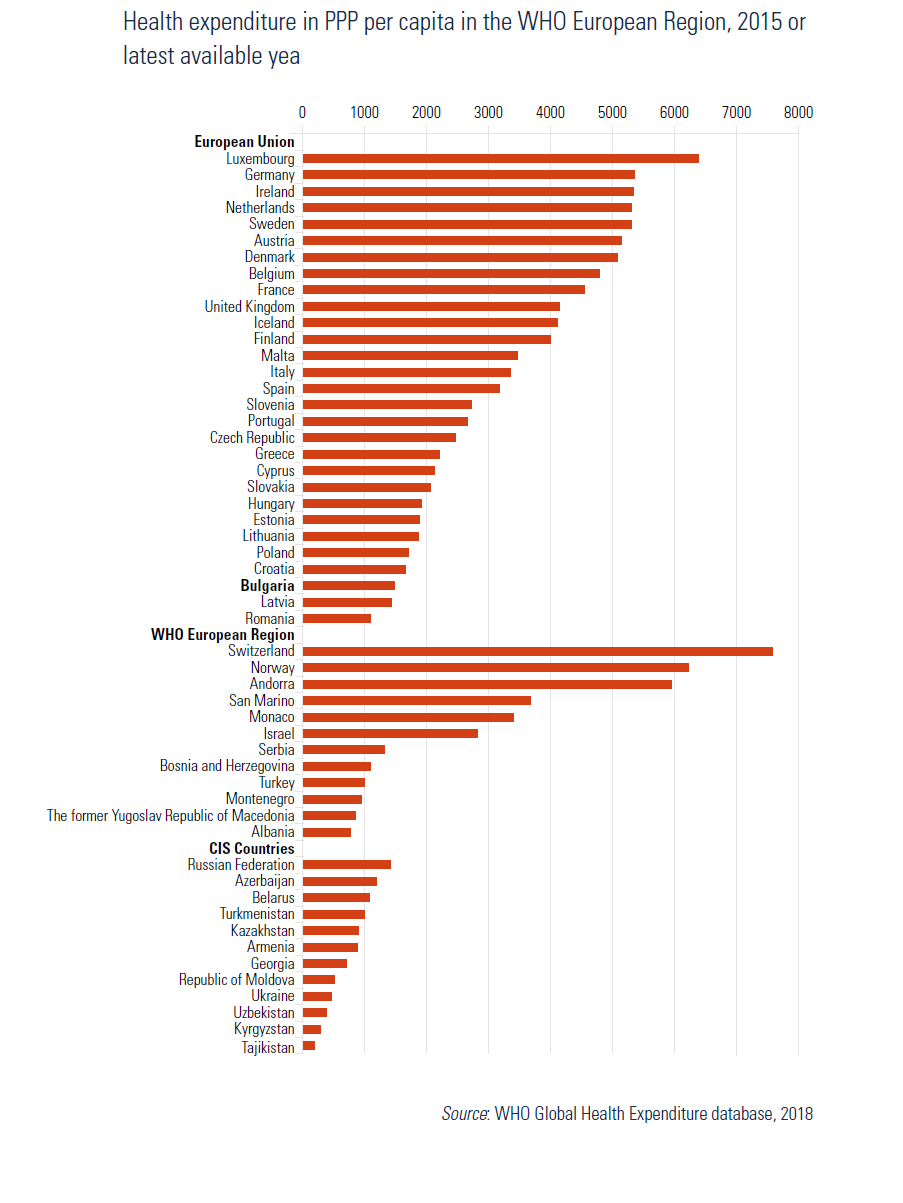
Per capita health expenditure increased threefold from 373 purchasing power parity in US dollars (US$ PPP) in 2000 to US$ 1492 PPP in 2015, reflecting both the GDP growth and total health expenditure growth as a percentage of GDP (Table1.2 and Table3.1). Hence, the gap between the Bulgarian per capita health expenditure and the EU average has decreased in the last 15 years. However, the Bulgarian per capita health expenditure was still below the EU28 average (US$ 3310 PPP) in 2015 (WHO, 2018). Among EU Member States, only Romania and Latvia have a lower per capita health spending than Bulgaria in 2015 (Fig3.4).
| Table1.2 | Fig3.4 |
 |  |
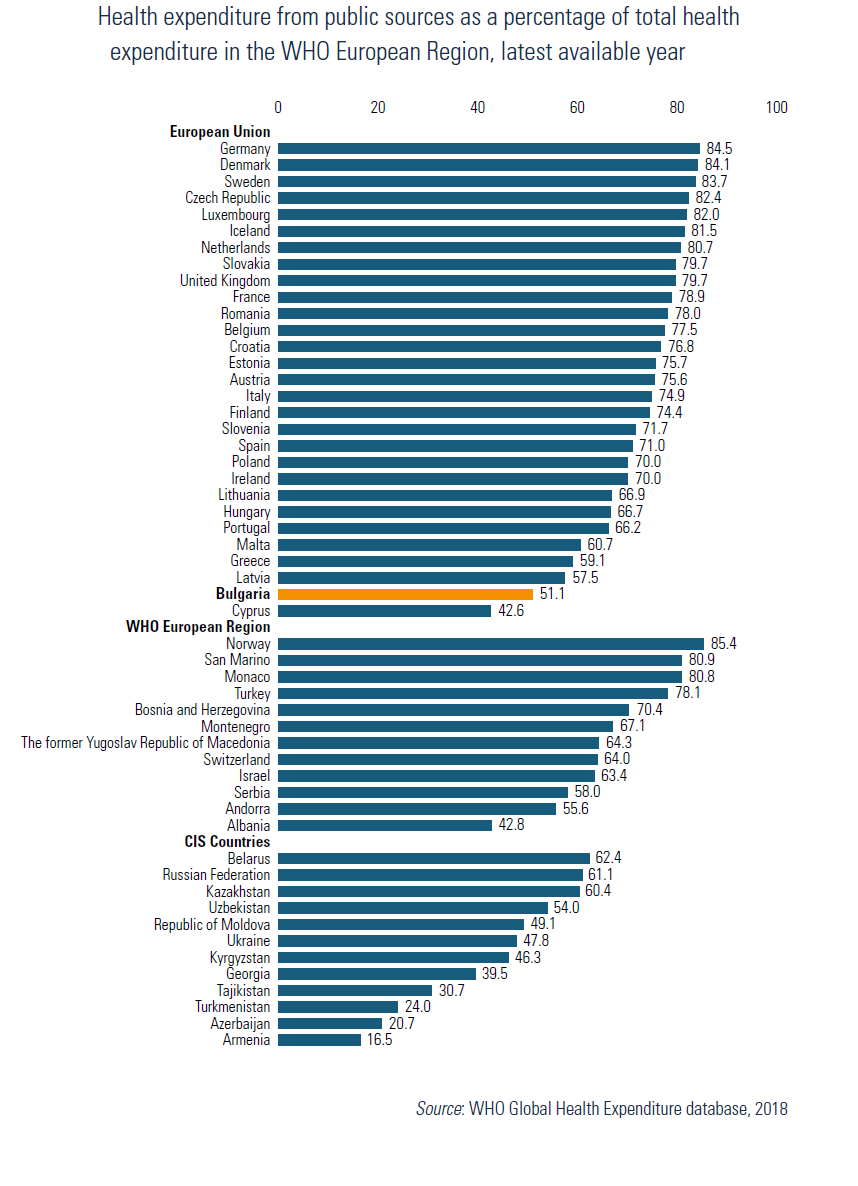
While general government health expenditure as a percentage of GDP has remained relatively constant (around 4%) between 2000 and 2015 (Table3.1), the share of the private, mainly OOP, expenditure grew from 2.2% in 2000 to 3.9% of GDP in 2015 (Eurostat, 2018). Although both public and private health expenditure increased in absolute values, the growth rate of private expenditure outpaced that of public spending. Private expenditure on health as a percentage of total expenditure has grown from 39.1% in 2000 to 48.9% in 2015 (Table3.1), which is the second highest value in the EU after Cyprus. Comparing only OOP expenditure, Bulgaria has the largest share among all EU Member States (47.7% of total health expenditure in 2015; Eurostat, 2018). Meanwhile, public expenditure on health as a share of total health expenditure has gradually decreased during the entire transition period from officially 100% in 1989–1990 to 51.1% in 2015 (WHO, 2018). From an international perspective, Bulgaria’s public share of health expenditure was below all except two European and nine Commonwealth of Independent States countries in 2015 (Fig3.5).
Fig3.5
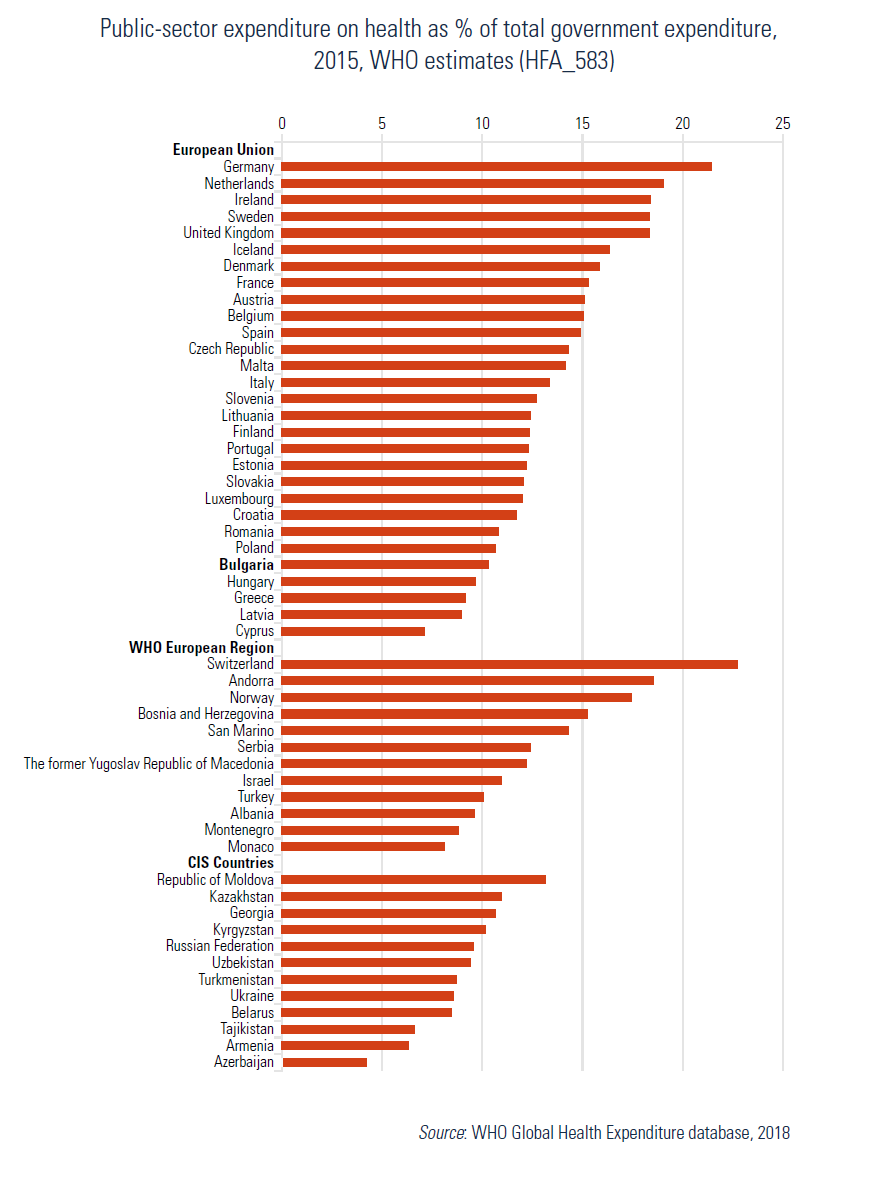
Public expenditure on health as a percentage of the total government spending (10.3% in 2015) was comparable with the newest EU Member States (Fig3.6) but lower than the EU average (15.3% in 2014). This indicator reached its lowest value after 2000 in 2009 (9.1%) probably reflecting government priorities facing the economic crisis (WHO, 2018).
Fig3.6
The trend of private (mainly OOP) expenditure increasing as a share of total health expenditure is stable, with some variations over the years. This might be to the result of a shortage or inefficient use of public resources for health care, considering the fact that the public expenditure per capita tripled from 2000 (US$ 223 PPP) to 2015 (US$ 762 PPP) (WHO, 2018).
Public expenditure on health consists of health spending by the NHIF, the government (MoH, ministries operating parallel health systems, and the central budget) and municipalities. The share of each public source in total public expenditure on health changed during the transition period. The share of SHI expenditure has increased gradually since 2000 and represents the largest public source of health care funding. In 2015, it stood at 41.9% (up from 31.6% of the total current health expenditure in 2004; WHO, 2018). Simultaneously, general government expenditure as a share of the total health expenditure decreased from 26.3% in 2005 to 10.3% in 2015 (Eurostat, 2018).
Approximately half of current health expenditure is spent on curative and rehabilitation services (Table3.2), varying between 51% and 54% in the period 2003–2010 and declining to 48–49% in 2011–2015. Whereas the share of inpatient curative and rehabilitative care declined from 41.1% of current health expenditure in 2008 to 29.4% in 2015, the share of outpatient curative and rehabilitation care expenditure remained relatively stable around 14%, and the share of curative and rehabilitation day care expenditure increased to 4.7% in 2015.
Table3.2

Expenditure on medical goods (pharmaceuticals and therapeutic appliances) ranks second as a share of total health expenditure (Eurostat, 2018). The share spend on medical goods grew from 38.5% in 2003 to 40.7% of total health expenditure in 2015, more than 95% of which being spent for pharmaceuticals. As a result, pharmaceutical expenditure per capita (€498 purchasing power standard) was the fourth largest in the EU after Germany, France and Belgium in 2015 (Eurostat, 2018). The growth of pharmaceutical expenditure both in absolute value (tripling from 2003 to 2015) and as a percentage of total health expenditure is substantial and has the greatest impact on OOP expenditure increase, considering the fact that pharmaceuticals account for the largest share of OOP expenditure (on average 67% for 2003–2015). Traditionally, nearly 80% of pharmaceutical expenditure is OOP (Eurostat, 2018), which makes the public coverage for pharmaceuticals in Bulgaria the lowest in the EU, except for Cyprus (OECD/EU, 2016).
Although public health services, prevention and health promotion are acknowledged as a priority by all health authorities, their corresponding share in current health expenditure is small and declined further to less than 3% in 2013–2015 (Eurostat, 2018). However, in absolute value, expenditure on prevention and public health services increased each year since 2003 (except in 2009 – not shown in the table), reaching its peak in 2010. The expenditure on prevention and public health services in absolute value were nearly two times higher in 2015 than in 2003 (Eurostat, 2018).
In late March 2025, Parliament approved the National Health Insurance Fund (NHIF) budget for 2025 alongside the state and social security budgets. The NHIF budget, set at €4.7 billion, reflects a 16% increase compared to 2024, though its expenditure structure remains largely unchanged. The largest allocation (€2.1 billion, or 46.8% of total spending on services and goods) is directed toward inpatient care, followed by pharmaceuticals and medical devices at €1.2 billion (26.7%). Primary outpatient care and specialized outpatient care each receive slightly over 7% of the total expenditure.
The 2025 budget also introduces new measures, including full reimbursement for prescribed antibiotics and antiviral medications for children up to seven years of age (see also the policy analysis “Introduction of public coverage for antiviral drugs and antibiotics for children”); coverage of biomarker testing costs for cancer diagnosis and financial support for pharmacies operating in remote or underserved areas.
Authors
References
The 2021 National Health Insurance Fund budget bill envisions increases by nearly 13% in revenues and expenditures without significant structural changes.
On the revenue side, a total amount of BGN 5,341 billion (EUR 2,670 billion) is expected (an increase by BGN 567 million (EUR 283 million) compared to 2020). Similar to 2020, the excess is warrantable by the expected increase of the employees' insurance income and the increase of the insurance income base for the state's contributions.
The NHIF will receive an additional BGN 237 million (EUR 118 million) from the Ministry of Health. This money is earmarked to cover the supplement to the medical staff's salaries for the epidemic emergency duration. Physicians will receive additional BGN 600, nurses BGN 360, and medical orderlies BGN 120 per month. Physicians with monthly salaries exceeding BGN 5000 will not be eligible for the supplement.
Traditionally, the largest share of expenditures is allocated to inpatient care: BGN 2,645 billion (EUR 1,322 billion), which exceeds the previous years by 17%. The next most significant line item is the projected expenditure on medicinal products amounting to BGN 1,332 billion (EUR 666 billion). Compared to 2020, the growth in this expenditure item is 7%.
There is a growth in the amounts allocated for primary outpatient medical care, specialized outpatient medical care, and outpatient diagnostic services. Despite the increase, this line-items continue to constitute only about 12% of the total NHIF expenditures.
The bill also empowers the Council of Ministers to approve additional transfers to the NHIF for COVID-19-related activities.
Authors
References
Law on the 2020 NHIF’s Budget, https://www.lex.bg/bg/laws/ldoc/2137198374 (in Bulgarian)
Law on the 2021 NHIF’s Budget, https://www.lex.bg/bg/laws/ldoc/2137207515 (in Bulgarian)
The 2020 National Health Insurance Fund (NHIF) budget shows a further increase in both revenues and expenditures, although there are no significant changes in the structure of expenditures. Unlike previous years, the expected growth of inpatient care expenditures is mainly due to an increase in prices of clinical pathways rather than the increase in the volume of hospitalizations. However, the budget also envisions a higher volume of primary and outpatient care activities such as health promotion, prophylactic, and diagnostic services.
Expected revenues for 2020 are BGN 4,745 billion (EUR 2,426 billion, increase by BGN 445 million (EUR 227 million) compared to 2019). The excess is warrantable by the expected increase of the employees’ insurance income and the increase of the insurance income base for the contributions paid by the state.
Similar to previous years, the most significant share of expenditures (47%) is distributed to inpatient care: BGN 2,247 billion (EUR 1,149 billion), which exceeds the previous years’ by 12%.
The next significant share of the expenditures (26%) with the second biggest growth rate, compared to the previous year (11%), is the amount for medicinal products. NHIF plans to spend BGN 1,243 billion (EUR 636 million) in this line-item. This growth is justified mostly by the increase in the amount allocated for reimbursing oncological drugs.
There is a less pronounced expenditure growth for primary outpatient medical care, specialized outpatient medical care, and outpatient diagnostic services. The increase of these expenditures is reflecting the recent revision of the scope of the benefit package. The new decree, issued by the Ministry of Health, envisions growth in the volume of prophylactic, diagnostic, and other outpatient services aiming to constrain unnecessary hospitalizations.
Despite the growth of funds allocated to prophylactic and diagnostic services, they still represent only 12% of NHIF’s total spending.
Authors
References
Law on the 2019 NHIF’s Budget, https://www.mh.government.bg/media/filer_public/2018/12/11/zakon-budvet-nzok-2019.pdf (in Bulgarian)
Law on the 2020 NHIF’s Budget, http://www.mh.government.bg/media/filer_public/2019/12/17/zakon-budjet-nzok-2020.pdf(in Bulgarian)