-
17 September 2025 | Policy Analysis
State of progress of the hospital landscape reform: A working group with independent experts -
15 June 2023 | Country Update
Implementation of hospital at home for cancer treatment and antibiotic therapy -
27 March 2023 | Country Update
A further step towards centralised care in reference centres -
25 July 2022 | Policy Analysis
State of progress of the hospital reform: the assignment of care missions to hospital networks
5.4. Specialized ambulatory care / inpatient care
Every citizen has access to medical specialists without a referral. In particular for gynaecology, ophthalmology, dermatology, paediatrics and otorhinolaryngology care, patients tend to go directly to the medical specialist instead of their GP.
Hospital at home (HAH) consists of delivering care in the patient’s place of residence that would otherwise need to be delivered in an acute hospital. HAH pilot projects were already launched in March 2017, but from July 2023, HAH will be rolled out on a more structural basis in the fields of oncology and antibiotic therapy for relevant patients.
HAH is selected by the hospital’s medical specialist in consultation with the patient, their GP and a home nursing team. All parties involved have to agree on a care plan. The hospital pharmacist is responsible for preparing, transporting and delivering the medication (if the patient has a reference pharmacist, they are also kept informed) and the collection of high-risk medical waste is the hospital’s responsibility. The budget impact of this initiative is neutral both for the national health insurance and for the patient (they do not pay more).
Authors
References
5.4.1. Specialized ambulatory / outpatient care
Medical specialists can work on an ambulatory basis in hospitals (public or private not-for-profit),[12] in private for-profit clinics (called extramural centres, see Box5.4) and/or in a private practice.
In hospitals, medical specialists can hold their ambulatory consultations in the polyclinic, which is a space in the hospital separate from inpatients, and can combine this with consulting in their private practice or in extramural centres.
In ambulatory settings, medical specialists are paid on an FFS basis and patient co-payments are higher than for GP consultations. Some specialists did not agree or only partially agreed to the national official tariffs, indicating that they may charge extra-billings (see Section 3.3.4 for more details) (IMA-AIM, 2019a). There is no registered information on the amount of extra-billings charged to patients in ambulatory settings. In the case of hospitalization, a recent study showed that the amount of extra-billings charged to patients in single-bed rooms increased, potentially due to the ban on charging extra-billings for double or multiple-bed rooms (IMA-AIM, 2019c).
- 12. To be considered as a hospital, the law stipulates that it can either be public or private not-for-profit. For-profit institutions are not considered as hospitals. ↰
5.4.2. Inpatient care
Inpatient care refers to a patient admitted into a licensed hospital, public or private, who is not discharged on the day of admission. According to the Belgian Hospital Act, several standards and criteria have to be met for a health care establishment to be licensed as a hospital (see Section 2.4.2) (Justel 7 November 2008). A hospital consists of hospital services including medico-technical services (such as imaging and radiotherapy), hospital departments, hospital functions and care programmes. Hospital functions are transverse; that is to say, they are not aimed at a specific patient group and extend across the different services of the hospital (pharmacy, palliative care, blood bank, intensive care, emergency care). A care programme is a coherent set of care services working in a multidisciplinary and transverse way for a well defined target patient group (such as reproductive medicine, cardiology, oncology, paediatrics and geriatrics). A distinction is made between basic care programmes for regular conditions and specialized care programmes for rarer conditions, which are not available in every hospital (BS-MB 8 August 2014a). Licensing criteria are defined for the different services, departments, functions and care programmes. For several services, functions and care programmes, there are also programming criteria based on a national planning (see Section 2.4.2) (MoH, 2016c).
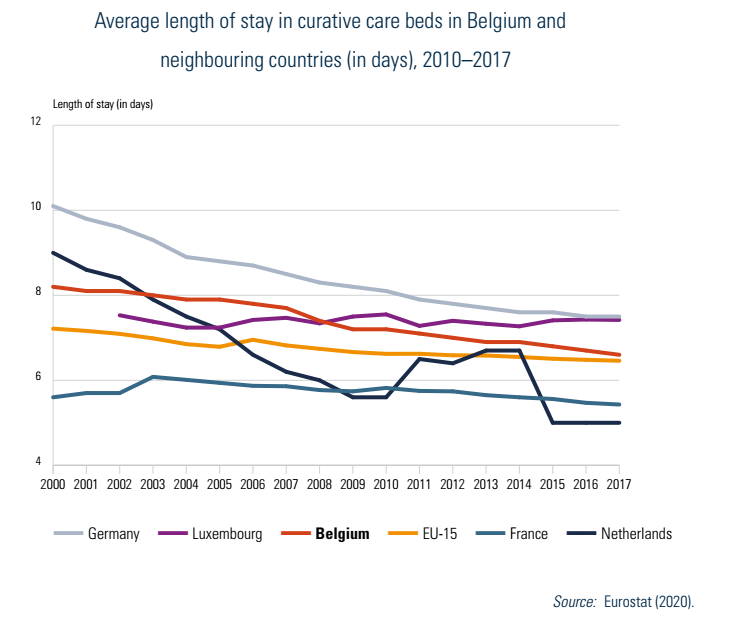
Length of inpatient stays
Between 2000 and 2017, the average length of stay (ALOS) in inpatient curative care beds decreased from 8.2 days to 6.6 days, which is in line with neighbouring countries (see Fig5.2). Multiple factors have contributed to the decrease over time, including financial incentives to increase efficiency and shorten stays, medico-technical progress, the development of home care services and the expansion of day care. A projection study predicted a further reduction of ALOS to 5.94 days in 2025 (Van de Voorde et al., 2017).[13] Examples of initiatives to decrease length of stay concern the inpatient stays of women with normal deliveries (see also Box5.5). The ALOS for a normal birth is considered an appropriate indicator for the efficient use of health care services due to the comparable case-mix of patients. In Belgium, the ALOS for a normal birth decreased from 4.96 days in 2010 to 3.11 days in 2016, which is now close to the EU15 average (2.8 days in 2016; data available for 13 countries).
Fig5.2
Initiatives on inpatient care
Since 2015, an Action Plan of both the Federal State and Federated entities to reform the current hospital landscape has been drafted (see Chapter 6) (Van de Voorde et al., 2014, 2017). Initiatives on care concentration, including referral agreements, are in progress. For example from January 2020, complex surgery of the pancreas and oesophagus are only reimbursed in a limited number of hospitals with proven experience (NIHDI, 2019c). There are also initiatives to stimulate the integration of care between settings (see Box5.5).
Quality of inpatient care
Quality criteria are embedded in the licensing criteria specific to hospital services, departments, functions and care programmes. Inspection ensures that hospitals comply with these quality criteria at the levels of structure, processes and results. Since the 6th State Reform (1 July 2014), assessing the quality of a hospital is an exclusive competence of the Federated entities. However, if they decide to establish new criteria, they may not impact the Federal competences or impact the Federal budget.
In Flanders, inspections are performed unannounced, whereby a care trajectory of a certain type of patient is followed. In addition, the Flemish Indicators Project for Patients and Professionals (VIP2) measures the quality of care in most Flemish general hospitals. The hospitals choose which indicators they measure. Results appear (if the hospital agrees) on a website www.zorgkwaliteit.be (Flemish Agency for Care and Health). The German-speaking community regularly organizes announced quality inspections in hospitals in collaboration with the Flemish organization. In Brussels and the Walloon region, the organization Plateforme pour l’Amélioration continue de la Qualité des soins et de la Sécurité des patients (PAQS) has set up quality indicators in close collaboration with the sector for benchmarking (each hospital receives its own results compared to the average) (PAQS, 2018). Nevertheless, these data are not yet collected in a systematic way. In the case of hospital accreditation, which is voluntary, an external organization assesses the extent to which the hospital offers quality and safe care. Since 2008, hospitals can receive accreditation for a limited number of years, with an increasing number of hospitals obtaining accreditation (58% in 2019) or in the process of obtaining accreditation (27% in 2019).
Since 2018, a P4P programme for general hospitals also grants an additional budget to hospitals that score well on an indicator set of four hospital-wide and seven pathology-related indicators (see Section 6.1). Participation is voluntary.
Quality initiatives concerning the measurement of patient experiences are described in Box5.6. Additional quality initiatives are described in Box2.4 in Chapter 2.
- 13. For acute and chronic inpatient care. ↰
Context
A redesign of the hospital landscape has been underway for several years, exemplified by the creation of local hospital networks under the law of 29 February 2019 (see the policy analysis of 25 July 2022). Since early 2025, the debate surrounding hospital landscape reform has intensified. In response to key challenges, including the rise of outpatient care, low acute bed occupancy rates, fragmented services and staff shortages, the Interministerial Conference on Public Health of 24 March 2025 decided to establish a working group of independent experts tasked with developing in-depth recommendations for the future organization of hospitals.
Main purpose and tasks assigned to the group of experts
The group of experts will explore restructuring options guided by the principle: “local care when possible, centralised care when necessary.” This also includes defining the roles of institutions, improving infrastructure use and fostering hospital collaboration.
The initial focus will be on acute somatic care. Belgium has 103 general and academic hospitals, some with multiple sites. The group of experts will assess how to differentiate their missions and improve collaboration to enhance care quality and resource efficiency, while balancing geographic accessibility and care concentration.
If feasible, the mission of the experts group may also be expanded to
- include an evaluation of the current 25 local hospital networks to enhance inter-hospital cooperation,
- address the integration of acute, chronic, rehabilitation and mental health care,
- reflect on the organization of acute psychiatric care, including bed numbers and distribution, and
- address the optimization of patient care pathways.
Outcomes
A report with recommendations is expected by the end of 2025.
Authors
References
A study of the Belgian Health care Knowledge Centre performed in collaboration with the Belgian Cancer Registry and clinical experts, published on 16 March 2023, has shown that breast cancer patients have a higher chance of survival when they are treated in a breast clinic that is specifically recognised for the treatment of this type of tumour. Therefore, the National Institute For Health and Disability Insurance plans to adapt the reimbursement rules so that only recognised breast clinics can offer certain reimbursed treatments to breast cancer patients.
Authors
On 20 July 2022, the Council of Ministers approved a draft of the Royal Decree qualifying supra-regional and loco-regional care missions for loco-regional hospital networks. As explained in the policy analysis of 19 October 2019, the law of 28 February 2019 provided for the creation of 25 loco-regional hospital networks by 2020. A draft of the royal decree now lists the loco-regional care missions that will have to be offered in each network and the supra-regional care missions that cannot be offered in each network.
The listed loco-regional care missions must be provided in each loco-regional network, possibly through collaboration agreements, but not necessarily in each hospital of the network. Geographical criteria have nevertheless been defined, that is, each listed loco-regional mission must be offered by the network in such a way as to ensure that 90% of the citizens in the geographical area covered by the network have a maximum travel time of 30 minutes (by ordinary vehicle under normal traffic conditions on an average weekday). The rule of 30 minutes can be waived if, in order to guarantee the travel time, investments in real estate infrastructure are required in a new location or if the care mission is offered in a neighbouring loco-regional network within 30 minutes. This list concerns not only missions where emergency care is required, but also, those that the patient frequently needs (such as radiotherapy) or situations where a long stay and frequent visits by the patient’s family may be needed (for example, paediatric or geriatric care). This list is dynamic and will evolve according to scientific developments. Each network will have three years to comply with the travel time criteria.
The list of supra-regional care missions that cannot be offered in each network concern:
- the care missions related to services for contagious diseases, intensive neonatology, and tuberculosis treatment,
- the functions of regional perinatal care, rare diseases, and paediatric liaisons;
- the care missions of the centres of expertise for comatose patients, burns, or transplantations;
- the medico-technical services of nuclear medicine in which a PET-scan is installed;
- the centres of human genetics recognized as heavy medico-technical service; and
- care programs for paediatric haemato-oncology, cardiac surgery, heart and heart-lung transplantation, children with congenital cardiac anomalies, children with congenital heart defects, electrophysiology, reproductive medicine and acute stroke care involving invasive procedures.
Authors
References
CMR 2022. Ontwerp KB/Projet d’AR van/du 20-07-2022 (2022A71750.019). (https://gcm.rmnet.be/clients/rmnet/content/medias/3_ontwerp_kb_loco_supra__1_.doc).
News. Belgium 2022. Qualification des missions de soins des réseaux hospitaliers cliniques locorégionaux (Qualification of the care missions of loco-regional clinical hospital networks). Brussels: Council of Minister of 20 July 2022 (https://news.belgium.be/fr/qualification-des-missions-de-soins-des-reseaux-hospitaliers-cliniques-locoregionaux).
MediSphère 8 June 2022. Trentes minutes maximum pour aller à l’hôpital: les réseaux hospitaliers s'inquiètent. (Thirty minutes maximum to go to the hospital: hospital networks are worried) (https://www.medi-sphere.be/fr/actualites/30-minutes-maximum-pour-aller-a-l-rsquo-hopital-les-reseaux-hospitaliers-en-difficulte.html).
5.4.3. Day care
In Belgium, the formal description of day care is day hospital and is only reserved for licensed hospitals (BS-MB 5 December 1997; BS-MB 7 March 2008), with established procedures for selection of patients, safety, quality control, continuity, reporting and cooperation with various medico-technical services (NIHDI, 2013). It can be for a surgical intervention (called surgical day care) or a number of diagnostic tests, therapeutic tests, or oncological therapies (called medical day care).
Technical acts that are performed in a consultation room or the consultation ward of a polyclinic (such as suturing wounds), as well as care acts performed in a private clinic (such as refractive eye surgery) are considered ambulatory care and not day care. Some acts (such as surgical tooth extraction) can be performed both in ambulatory and day care settings.
The proportion of day care admissions represented 60.6% of all general hospital stays in 2014. In the period 2008–2014, day care admissions showed an average annual growth rate of 4.3%. Most day care admissions were for non-surgical procedures (including intravenous therapy and chemotherapy), representing 78% of the number of day care admissions in 2014 (Van de Voorde et al., 2017).
The shift to day care varies between hospitals and between interventions. Some incentives have been introduced to promote day care. However, the payment rules are complex (some interventions are financed within a closed-end budget and others, on a nominative list, are paid for by lump sums) and lack transparency. As a consequence, they fail to give clear incentives to health care providers. Additional mechanisms are needed to both encourage day surgery and avoid a suction effect on procedures that could easily be performed in the doctor’s consultation room; see the KCE Report 282 for more details on day care (Leroy et al., 2017).
A trend analysis for planning hospital capacity for 2025 concluded that more beds for day care will be necessary (Van de Voorde et al., 2017).