4.1. Physical resources
4.1.1. Capital stock and investments
Current capital stock
There are four licensed public hospitals, of which two are acute hospitals and two are specialized hospitals in oncology and rehabilitation respectively. There are six licensed private hospitals, four licensed private day-care clinics, and nine licensed mental health facilities. All hospitals are located in Malta with the exception of one hospital located on the island of Gozo (see Box4.1). The majority of patient services were moved from St Luke’s Hospital to Mater Dei Hospital (MDH) in November 2007; MDH is an acute general teaching hospital offering a full range of services.
Box4.1

Founded in 1990, the Foundation for Medical Services is a public entity managing capital projects. It was responsible for the construction and commissioning of MDH and the Sir Anthony Mamo Oncology Centre (SAMOC) located adjacent to it. The Foundation has recently overseen the construction of the SAMOC – a project part-financed by the EU through European Regional Development Funds, among other development projects. This led to the migration of oncology services from the old Sir Paul Boffa Hospital to MDH and SAMOC, thus further centralizing health care operations.
The Foundation for Medical Services typically appoints the head of public hospitals’ management teams and there has been a trend to appoint nonclinical people to the position of Chief Executive. Recently, there have also been efforts to involve clinicians in the management of clinical services. In contrast, private hospitals are managed by individual, for-profit companies.
MDH and SAMOC are modern hospitals that have been built within the last 10 years, whereas the other hospitals were built during the 20th century. Hospitals in the private sector have been built during the past 20 years.
Regulation of capital investment
To date, once a new hospital application fulfils the necessary requirements and standards, there is no capping on the number or geographical distribution of facilities, unlike that for pharmacies. Public primary health care has struggled because of chronic underinvestment during the period that MDH was being developed. Since 2010 several refurbishment initiatives have taken place in health centres, for example the Rabat and Mosta Health Centres. A plan has been developed for a new Paola primary health care facility.
Investment funding
Investment is generally financed by national public funds generated through taxation. However, EU membership has created opportunities for investment funding using European Regional Development Funds.
Since 2013 the Government has embarked on an initiative to use private capital investment to modernize the existing capital stock through strategic collaboration with a private partner. This is a new model for the Maltese health care system. The selected private company will invest capital and in return acquire ownership of St Luke’s Hospital, Karin Grech Rehabilitation Hospital and Gozo General Hospital for a period of 30 years. In addition, there has been a continuation of public–private partnerships within the long-term care sector, where several variations of public–private associations exist, ranging from models whereby hotel and infrastructural services are provided by the private sector, while social and health care provision is funded by public sources through procurement of the full long-term care service at an established per diem rate.
There is no money borrowed through public allocation earmarked for the health care sector.
4.1.2. Infrastructure
The total number of beds per capita has increased in recent years both in acute care hospitals and in long-term care facilities. The switch of designation of St Vincent De Paul Residence, the main geriatric facility, from ‘nursing home’ status to a specialty hospital and then back to a nursing home accounted for earlier substantial shifts in long-term capacity statistics. The building of the new SAMOC has also increased the number of beds available as a result of Boffa Hospital being restructured and refurbished to accommodate patients for long-term care.
Changes in the mix of beds are partially due to restructuring, such as shifting the main state general hospital’s (St Luke’s Hospital) capacity to the new MDH in 2007; a number of beds were retained as long-term or rehabilitation beds in Karin Grech Rehabilitation Hospital within the grounds of the old main general hospital. A decrease in the number of acute beds in 2005 was due to a change in the series definition.
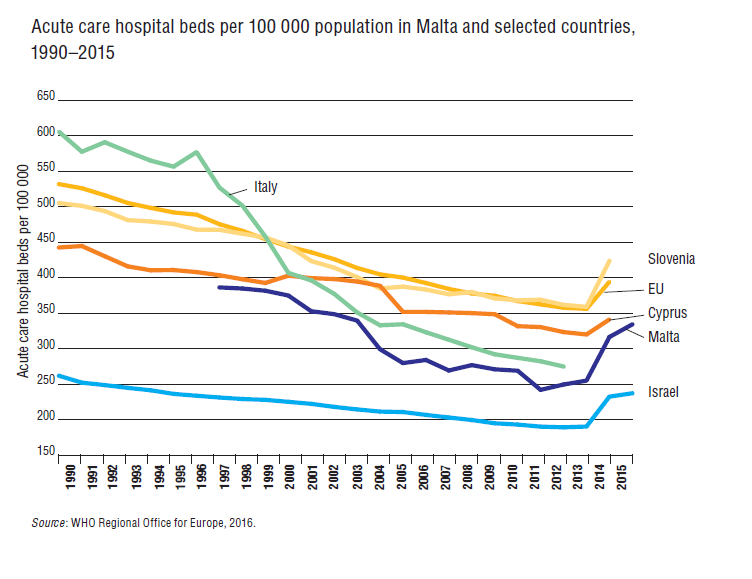
Malta has a higher bed occupancy rate in acute hospitals (81.8% in 2014) compared to the EU average (76.9% in 2014) (WHO Regional Office for Europe, 2016). One explanation for this higher occupancy rate is that the number of beds in acute hospitals is also below the EU average (Fig4.1). In fact, the number of acute care beds in Malta has increased from 279.8 per 100 000 population in 2005 to 334.4 per 100 000 in 2015, an increase of 20%. Average length of stay (ALOS) in acute hospitals has increased in recent years. This goes against the general trend of shorter lengths of stay across the EU. Nonetheless, although ALOS in Malta increased, it is still lower than the EU average.
Fig4.1
4.1.3. Medical equipment
Regulation of medical devices and aids
The Malta Competition and Consumer Affairs Authority (MCCAA) is the competent authority responsible for regulating medical devices and implementing the relevant EU Directives in this sector. HTA is, however, the remit of the Advisory Committee for Health Benefits within the Ministry for Health. Both public and private sectors have the same level of medical technology available at their disposal. There is no capping on investment in complex technology. Medical equipment is mostly hospital-based, but there is an increasing availability of medical imaging devices such as X-ray machines at specific primary health care centres on a 24-hour basis and in private clinics.
Equipment infrastructure
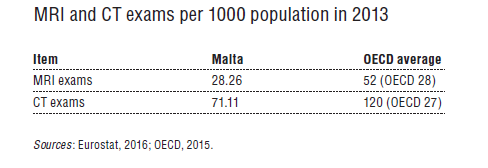
In terms of CT exams per 1000 inhabitants, Malta is comparable to the Netherlands and Croatia. The number of MRI scans per 1000 inhabitants is higher than in Cyprus and lower than in Greece. When compared to the OECD average, Malta has a low number of both MRI and CT exams per 1000 population (Table4.1). Due to the fact that there are two PET scanners (one in the public and the other in the private sector), Malta emerges as having a high ratio of PET scanners per capita when compared to other countries (Eurostat, 2016b).
Table4.1
4.1.4. Information technology and eHealth
In 2014, 73% of the Maltese population had used the Internet within the last three months, while 53% reported accessing the Internet for health information (Eurostat, 2016b).
Since the early 1990s there has been steady growth in the use of IT throughout the health system, and this is most evident in public secondary care. In particular, the implementation of the Health-Care Information System in 1997 and the first phase of the Integrated Health Information System in 2007 led to noticeable penetration of IT infrastructure and applications throughout public hospitals and health centres.
Public hospitals and health centres have been operating an integrated appointment booking system since 1998. This has recently been integrated into the myHealth Portal.
In 2006 an eHealth Portal was launched. This facilitates access to specific health-related e-services, such as online referral to hospital, health information and information about government health services. In 2012 the myHealth system was launched which allows patients and the doctors they choose to gain direct access to their electronic patient record through the Internet, providing the first IT link between the private family doctor community and the public sector.
Uptake of the myHealth system increased considerably in 2016 following the introduction of a paper-based consent form and improvements in the user experience of the sign-up process, which practically facilitated uptake by patients and physicians alike. This resulted in a 681% increase in July 2016 (13 090) compared to September 2015 (1674) in the total number of patients who subscribed to the myHealth system and have been accepted by their respective doctors.
The development of health information systems at hospital level took a significant leap forward with the opening of MDH in 2007. Systems introduced include a radiology information system, a picture archiving and communication system, an integrated laboratory information system, and an order communication system. Since 2007 a number of additional systems have been introduced to cater for the increased demands within the health care systems, such as the Centralized Theatre Management System, Cardiovascular Information System (CVIS) and Online Surgical Register. In 2013 the old Patient Administration System was migrated to a new system known as the Clinical Patient Administration System (CPAS), which also acts as an electronic appointment booking system and is used nationwide through the health care system as a patient master index. In 2016 a Clinical Decision Support System, known as UpToDate, was implemented at MDH and SAMOC.
On a national level, in 2015 a Digital Health Portal was launched (http://digitalhealth.gov.mt) which intends to consolidate all online resources related to eHealth, such as the recently launched electronic Patient Referral Form, fast-track colorectal clinic referral form (authorized to trained GPs) and a number of paper-based forms which are used on a regular basis.
The nationwide deployment of the e-ID card that stores electronic identification data is well under way in mid-2016. This will allow secure identification and authentication of patients and health professionals, and hence facilitate authorization of online access to personal health data.
IT literacy and IT system use among private health care providers have also increased at a steady rate, but the use of electronic patient records by private family doctors has generally lagged behind and still depends largely on personal initiative. At this point, electronic patient records are only partially implemented at MDH and SAMOC, as the majority of clinical documentation is paper-based, with a number of units having their own electronic patient records, such as the CVIS within the cardiology department.
In 2015 the process commenced to apply for European Regional Development Funding through the 2014–2020 programme. If this project comes to fruition, it will enable the implementation of the next phase of the health information systems, which will include electronic patient records in the primary health care sector, electronic prescriptions, entitlement approval system, health data exchange, fully digitized patient registries and improved national electronic health records. An updated eHealth strategy is currently being developed and eHealth Week 2017 will take place in Malta during its Presidency of the Council of the EU.