3.3. Overview of the statutory financing system
3.3.1. Coverage
The SSN covers all citizens and ordinarily resident foreign nationals. Population coverage is automatic and universal. Undocumented migrants are entitled to access only urgent and essential services. Health care for prisoners, which was previously delivered through the Ministry of Justice, was integrated into the SSN in 1999; moreover, prisoners are usually excluded from having to pay co-payments.
In terms of the scope of coverage, the SSN guarantees the provision of health services included in the national benefits package (LEA) across the entire country. These are delivered through the activities of public providers (i.e. regional and local health care authorities, independent public hospitals (known as “hospital trusts”), university hospital trusts, the tertiary care and research centres (IRCCS) and private-accredited providers (see Chapter 2)). Regions can choose to offer non-LEA services but must finance these themselves. Health care services provided within the SSN (i.e. the LEA) are identified by positive and negative lists using criteria related to medical necessity, effectiveness, human dignity, appropriateness and efficiency in delivery (Lo Scalzo et al., 2009).
Positive lists exist for community care services (primary care, emergency care, pharmaceuticals, specialist outpatient care, integrated care, prosthesis care, ambulatory and home care, residential and semi-residential care, and thermal therapy), public health and occupational health services (Torbica & Fattore, 2005). For the latter, there is a list of general community and individual levels of preventive services that are covered, including hygiene and public health, immunization and early diagnosis tools. Hospital services are not specifically defined. Dental care – specifically orthodontics and dental prostheses – is generally not covered and is paid for out of pocket or reimbursed through policies offered by private for-profit and not-for-profit insurance companies (see Box3.1 and section 3.4).
Box3.1
Negative lists include ineffective services; services that are covered only on a case-by-case basis, such as orthodontics and laser eye surgery; and inpatient services for which ordinary hospital admissions are likely to be potentially inappropriate (e.g. cataract surgery and carpal tunnel release). For the latter category, regions should provide substitute treatment at other levels of the health care delivery system, such as day hospital and ambulatory care.
In 2017, the national benefits package was thoroughly revised and updated; in particular new vaccines, services for outpatient care, diagnostic services, neonatal care and health devices were added. It also included a list of rare disease to be covered by the SSN. Of note, Italy is probably the only country in Europe to introduce a voucher system to subsidize food for patients with coeliac disease.
3.3.2. Collection
The main source of financing for the Italian SSN is a mix of taxes applied at both regional and national level (see section 3.2). Thus, collection is performed partially at national and partially at regional level, although pooling of funds is managed at national level.
3.3.3. Pooling and allocation of funds
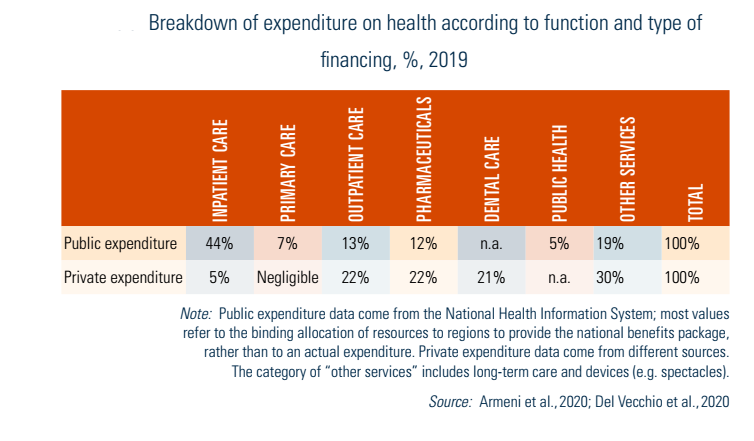
Each year the SSN’s health care funding is broadly allocated to three different areas of care that coincide with the main structural pillars of the national benefits package (LEA). In 2019, 5% of funding was allocated to prevention and public health services, 44% of funding was dedicated to hospital care and the remaining 51% to community care, which is further divided into primary care (7%), community pharmaceutical care (11.6%), specialist outpatient care (13.3%) and other district (community) health care (19.1%) (Table3.3) (Armeni et al., 2021). These values are used to allocate funding to the regions without, however, binding them to maintain such allocations. Regions are, in fact, free to reallocate the funds received within different programmes and to assign spending duties to local health authorities (as long as they adhere to delivering the national benefits package). In fact, while the central government regulates the national benefits package for citizens and controls the distribution of tax revenue, each region is individually responsible for the organization and delivery of services within its jurisdiction.
Table3.3
Each region has its institutional and organizational structure and thus determines the flow of resources within the system. The most common arrangement entails two main types of SSN organizations: local health authorities and hospital trusts (see Chapter 2). Local health authorities are generally funded according to a capitation formula, while independent public hospitals and private-accredited providers can be funded either directly by the region or by local health authorities according to a mix of per-case payments (Italian DRGs), fee-for-service (outpatient specialist care) and budget lines (fixed amounts of resources for specific duties or activities such as emergency care or organ transplantation services).
3.3.4. Purchasing and purchaser–provider relations
Regions differ in the purchasing models they implement. Some regions operate mainly integrated models (with hardly any purchaser/provider split), while others lean towards a more de-integrated model, with the extreme case of Lombardy where local health authorities (called health protection agencies, ATS) almost exclusively are purchasing organizations. Here we briefly discuss two examples in northern and affluent regions – Veneto (capital: Venice) and Lombardy (capital: Milan) – which operate integrated and contracting models respectively (Garattini et al., 2021; Bobini et al., 2020; Fattore, Numerato & Salvatore, 2022).
The Veneto regional health system serves around 5 million people and is structured into nine local health authorities which are divided into districts (26) where all community care services are delivered to patients. All but three SSN hospitals are run by local health authorities: the two largest general teaching hospitals and a specialized oncology hospital are independent organizations with their own senior managers. Hospital care is organized according to three tiers (hub, spoke and nodes), with the aim of ensuring continuity of care and promoting integration among different services. Administratively, the Veneto Region has consolidated several functions into a central operating agency to achieve economies of scale (Authorities Zero). Its activities include public procurement, regional labour contracts, HTA, capital planning, negotiations with private providers and clinical governance initiatives. Regional DRGs and fee-for-service schedules are used to allocate budgets within the local health authorities and to fund the three independent SSN hospitals as well as the few private-accredited providers operating in the region. The Veneto Region’s health system has been defined as “hierarchical” and benefits from the high level of technical and policy expertise of its bureaucracy (Bobini et al., 2020).
Since the late 1990s, the Lombardy Region has adopted a quasi-market approach for the delivery of hospital and outpatient care. In 1997 a major reform created a clear purchaser–provider split, strengthened patient’s freedom of choice of providers and fostered market competition, especially between public and private-accredited providers (Garattini et al., 2021). Currently the regional health system serves about 10 million people. It consists of nine health protection agencies that are in charge of purchasing virtually all services from 27 SSN delivery organizations, each one with its own territorial jurisdiction, three IRCCS, 29 accredited private hospitals and several accredited providers for community care. While the region is acknowledged as having an excellent hospital network, also evidenced by the high number of patients from other regions admitted to Lombardy’s private and public hospitals, the health system has also come under scrutiny by the central government for some features of its model that depart from national legislation. Moreover, a report released by AGENAS highlighted the excessive fragmentation of the governance system and recommended that the Lombardy Region strengthen the district organization of community care, clarify the roles of health protection agencies and reduce the number of SSN organizations acting in the system.
The reform of the regional health system was approved in December 2022 (Regional Law 22/2021). It transposes some of AGENAS recommendations, mainly to strengthen the role of community care, but leaves the fundamentals of the system substantially unchanged. In Lombardy’s regional health system, DRGs, fee-for-service schedules, and other mechanisms of funding related to sets of activities or care volumes play a larger role than in the Veneto Region due to the purchaser–provider split which is virtually complete in Lombardy and exists only to a modest extent in Veneto.[7] In addition, in Lombardy a higher share of the market is taken by private-accredited providers and the region emphasizes the role of patients’ choice. Nevertheless, over time the health protection agencies have increasingly engaged in targeted negotiations with both public and private-accredited providers over payments.
- 7. In Lombardy DRGs are the main source of funding of providers, while in Veneto DRGs are only used to fund the three independent SSN hospitals and accredited providers, as well as to compensate for the mobility of patients across jurisdictions. ↰