2.2. Organization
The French health care system is structurally based on a Bismarckian (SHI) approach, with goals of universality and solidarity that have led to an increasingly Beveridgian-type (NHS) system. The SHI currently covers 100% of the resident population (including undocumented migrants under certain conditions). Jurisdiction over health policy and regulation of the health care system (Fig2.1) is divided among:
Fig2.1
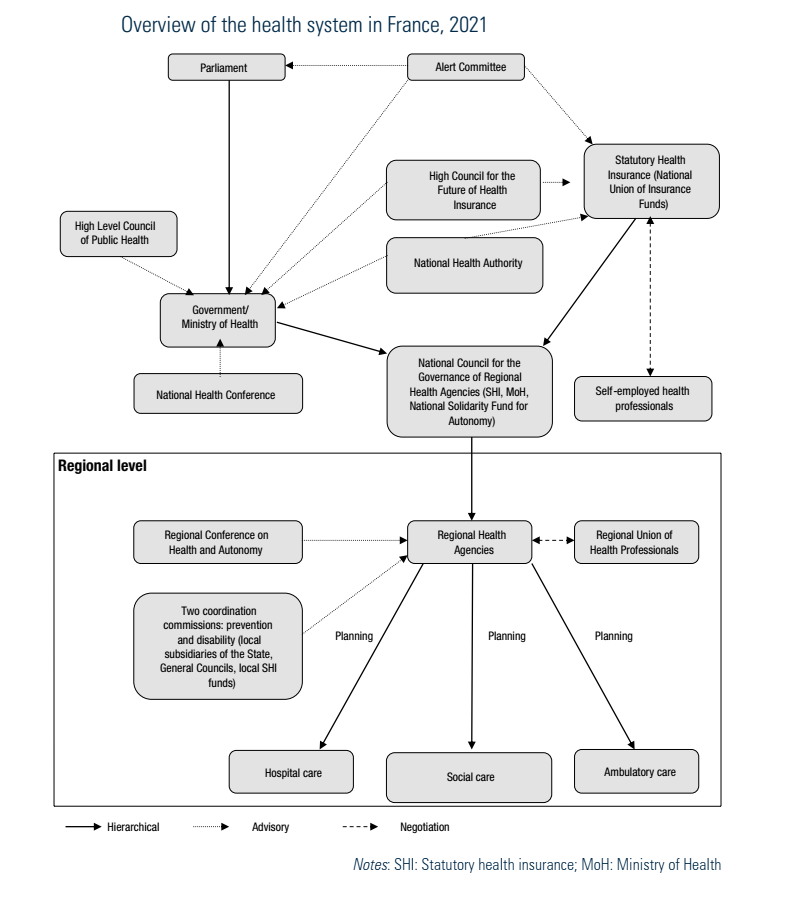
- the State: parliament and the government, specifically the MoH;[3]
- the SHI; and
- to a lesser extent, local authorities (départements).
Delivery of care is shared among private, FFS physicians and other health professionals, private for-profit hospitals, private non-profit hospitals and public hospitals. The current institutional organization of the health system is the result of the will of the founders of the social security system to create a single block system, guaranteeing uniform rights for all. Health insurance in France has, therefore, always been more concentrated and uniform than in other Bismarckian systems.
- 3. In this HiT, the Ministry of Health will refer to the administration of both health and social affairs (see section 2.2.2). ↰
2.2.1. The parliament
The parliament has control over the health care system via an annual Social Security Financing Act which sets a spending target for the health sector. It also influences health policy priorities by passing public health acts. The Social Security Financing Act is proposed by the government after a six-month preparation period in which all the directorates of the MoH are consulted as well as the Ministry of Finance; it is mostly based on proposals from the SHI Fund published in their yearly activity report (Rapport Charges et Produits). Several reports serve as a basis for discussion, including reports of: the National Court of Auditors (Cour des comptes), which is an independent public body responsible for monitoring state and social security bodies, to ensure adequate control over and proper use of public funds; the SHI; the High Council for the Future of Health Insurance (Haut conseil pour l’avenir de l’assurance maladie, HCAAM); and to a lesser extent the High Council of Public Health (Haut conseil de la santé publique, HCSP); and the National Health Conference (Conférence nationale de santé). The Social Security Financing Act:
- sets a projected target (ceiling) for health insurance spending for the following year, known as the National Objective for SHI Spending (Objectif national des dépenses d’assurance maladie, ONDAM);
- approves a report on trends in policy for health and social security; and
- contains new provisions concerning benefits and regulation.
The parliament also approves the revenue side of the budget based on the contribution rates for employers, beneficiaries and employees, and specific earmarked taxation proposed by the government.
The government, however, retains the leading role in proposing both public health and social security financing acts to the parliament and in writing the by-laws and decrees that result from the acts passed.
2.2.2. Ministry of Health (MoH)
The MoH is the central level of the Administration of Health and Social Affairs (Administration sanitaire et sociale). It comprises four directorates, which have the following responsibilities:
- General Directorate of Health (Direction générale de la santé, DGS), which oversees health policy;
- General Directorate of Healthcare Supply (Direction générale de l’offre de soins, DGOS), which manages the human and capital resources of the entire health care system;
- Directorate of Social Security (Direction de la sécurité sociale, DSS), which is responsible for the policies, governance and financing of the social security system, including preparation of the annual social security financing acts passed by the parliament; and
- General Directorate for Social Policy (Direction générale de la cohésion sociale, DGCS), which is responsible for health and social care for elderly, disabled and vulnerable people.
There is also a support directorate, shared between several ministries, that belongs to the public service of statistics and that is in charge of providing information and statistics on the system (Direction de la recherche, des études, de l’évaluation et des statistiques, DREES).
Depending on the government in place, the MoH has different names; it may include all four directorates or fewer – and each of the directorates will be under the responsibility of one or more ministers. This depends on the political power of the Minister who oversees health. For instance, after the election in 2017 the MoH had only one ministry grouping the four directorates and named the Ministry for Solidarity and Health (Ministère des solidarités et de la santé), while after the last election in May 2022 two ministries were created instead: the Ministry for Health and Prevention (Ministère de la Santé et de la Prévention) and the Ministry for solidarity, autonomy and disabled people (Ministère des Solidarités, de l’Autonomie et des Personnes handicapées).
The MoH is responsible for preparing and implementing government policy in the areas of public health, organization and financing of the health care system within the framework of the Public Health Act. It controls a large part of the regulation of health care expenditures on the basis of the overall framework established by the parliament. Its specific responsibilities include the following:
- allocating the budgeted expenditure among the different sectors (hospitals, ambulatory care, mental health care, etc.) and among the different regions;
- deciding on a pluri-annual number of health students to be trained in medical, pharmaceutical, dental and midwifery school each year, the number of hospital beds and the amount of equipment, including expensive medical technologies;
- setting the tariffs for public and private hospitals under the medical activity-based payment (ABP) system;
- approving the agreements signed between SHI and unions representing self-employed health care professionals (see section 3.7);
- setting the prices of medicines and devices on the basis of proposals from the French National Authority for Health (Haute Autorité de santé, HAS) ad hoc committees;
- establishing safety standards in hospitals; and
- defining priority areas for national health programmes.
At the regional level the Administration of Health and Social Affairs is represented by the ARS (see section 2.2.4), which are not directly under the supervision of the MoH but fall under the administrative supervision of the National steering council (Conseil national de pilotage, CNP), which is composed of delegates of the ministries in charge of health and in charge of public accounts and social security, the SHI and the National Solidarity Fund for Autonomy (Caisse nationale de solidarité pour l’autonomie, CNSA).
2.2.3. Other public agencies
The MoH relies upon a number of health agencies, which are under its supervision, and other public bodies in the development and implementation of policies for which it is responsible. Most of them are subordinate agencies with missions in a specific health area. These are:
- the French Biomedicine Agency (Agence de la biomédecine, ABM);
- the National Agency for Medicines and Health Products Safety (Agence nationale de sécurité du médicament et des produits de santé, ANSM);
- the French Agency for Food, Environmental and Occupational Health and Safety (Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail, ANSES);
- the National Agency to Support the Performance of Health and Health and Social Care Institutions (Agence nationale d’appui à la performance des établissements de santé et médico-sociaux, ANAP);
- the Technical Agency for Information on Hospital Care (Agence technique de l’information sur l’hospitalisation, ATIH);
- the French Blood Agency (Etablissement français du sang, EFS);
- the Radioprotection and Nuclear Safety Institute (Institut de radioprotection et de sûreté nucléaire, IRSN);
- the French National Cancer Institute (Institut national du cancer, INCa); and
- the French Public Health Agency (Santé publique France, SPF).
For more information on their missions see section 5.1.
Moreover, the HAS, an independent public body with financial autonomy, undertakes a number of activities designed to improve the quality of patient care. The HAS remit is diverse, ranging from assessment of drugs, medical devices and procedures to publication of guidelines, accreditation of health care organizations and protocols for recertification of doctors. It is mandated by law to carry out specific missions on which it reports to the government and the parliament.
2.2.4. Statutory health insurance (SHI)
The SHI is composed of three categories of schemes, which cover the entire population. Individuals and their families are affiliated with a scheme based on employment status. Working people have no choice regarding the scheme in which they are enrolled and may not opt out of coverage except in certain cases (for example, expatriates and employees of international corporations or institutions). Thus, there is no competition among the schemes. Persons who are not working are automatically enrolled in the general scheme, which is the major scheme.
The three categories of schemes and their beneficiaries in 2020 are approximately as follows:
- the general scheme (Caisse nationale d’assurance maladie, CNAM) covers everybody (around 88% of the population) except those eligible for other schemes (CNAM, 2021k);
- the agricultural scheme (Mutualité sociale agricole, MSA) covers farmers and agricultural employees and their families (around 5% of the population); and
- numerous “special schemes”, over 20 in number, built upon pre-SHI prepayment systems for defined categories of workers: local and national civil servants, miners, military personnel, employees of the national railway company, the clergy, sailors, the national bank, the gas and electricity company (they cover 7% of the population but technically manage claims and benefits for hardly 3%) (UNRS, 2022) (see section 3.3.1).
These schemes are federated into a National Union of Health Insurance Funds (Union nationale des caisses d’assurance maladie, UNCAM) for the purpose of representing the funds in negotiations with health care providers.
Each of the two major health insurance schemes is made up of a national health insurance fund and local structures corresponding to the degree of geographical distribution involved.
2.2.5. Professional organizations
There are two types of professional organizations: professional associations or councils (Conseil de l’ordre) and trade unions. For most medical specialties both an association and a union exist. Professional councils for doctors, pharmacists, dentists, midwives, physiotherapists and nurses are concerned with medical ethics and the supervision of professional practice. The council is responsible for all matters pertaining to the scientific activities of a specialty, including developing guidelines and ensuring compliance with annual continuing professional development (Développement professionnel continu, DPC) requirements, and from 2023 onwards recertification of some health professionals, while the union is in charge of the negotiations between the professionals and the SHI (see section 4.2.1) over fees and other matters affecting practice.
At the national level an umbrella organization represents all health care professionals in private practice: the National Union of Health Professions (Union nationale des professions de santé, UNPS). It sets the agenda for negotiations between health professionals and the SHI and CHI. Similarly, at regional level regional unions of health professionals (Unions régionales des professionnels de santé, URPS) negotiate with the ARS (see section 2.7.2).
In addition to their professional organizations and councils, health professionals may also join any of the trade unions that exist to represent workers in all fields of industry and services. In 2008 less than 20% of the health workforce were union members (Borgetto, 2008) – a rate which may have decreased since. Trade union representation is fragmented, not only because of the existence of different professions, but also through differences in status, for example, between salaried and self-employed professionals, or working in the hospital sector or not, or in the public or private sector. In addition to “vertical” unions, which represent interests at the national level, “horizontal” unions have developed at the local authority (département) level. As a result of this diversity, the unions’ positions on government measures may differ and decrease their power in negotiating. In 2021, as an attempt to partly solve this issue, a union of trade-unions of self-employed health professionals, “Les Libéraux de Santé” (“The self-employed”), was set up.