7.2. Accessibility
7.2.1. Population coverage and benefits basket
Overall, health care accessibility is high in France, with universal health insurance coverage and a broad and unique benefits basket for all residents. Financial accessibility is supported by a state-funded insurance which avoids cost-sharing for the poorest part of the population and for those with high health care needs (see section 3.3.1).
Nevertheless, the existence of cost-sharing for most services creates the need to pay for CHI, which can constitute significant spending for low-income households. Recent reforms have pushed for increased regulation of CHI contracts so that they cover 100% of the cost of a range of services with regulated prices, including basic dentures, hearing aids and optical care, resulting in a better coverage of these services (see section 7.3).
7.2.2. Availability of services
Despite the relatively high number of health care providers in France, geographical accessibility of health care, in particular primary care, remains a persistent problem for ensuring equal access to care (see Box4.2). Health care professionals are free to decide where to establish their practice and are highly concentrated in urban and coastal areas. Financial incentives to attract physicians to underserved areas have had limited success. While the creation of multidisciplinary primary care group practices has shown potential to attract younger physicians to underserved areas (Chevillard & Mousquès, 2021), these measures have not been sufficient for increasing primary care accessibility.
Box4.2
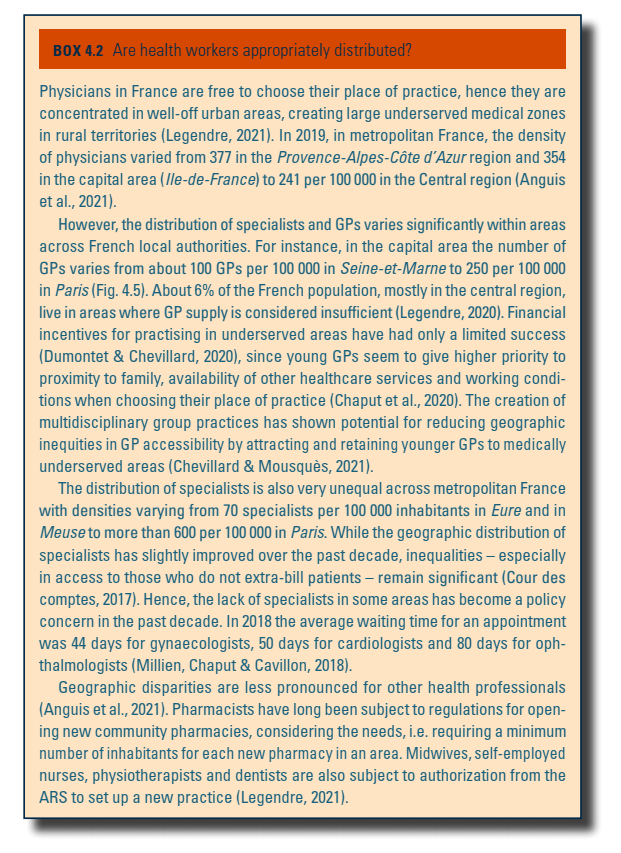
Hospital bed capacity is high in France compared to the OECD average (OECD, 2021a). The overall accessibility of hospital care is also high despite variations in the density of different types of hospital bed across regions, with, for instance, a higher hospitalization at home capacity in the capital region, and higher psychiatric hospital capacity in rural areas. Around 95% of the French population can equally access hospital care in less than 45 minutes by road (75% in less than 25 minutes) and 90% of the population has access to emergency care in less than 30 minutes (AMRP, 2021; Coldefy, Com-Ruelle & Lucas-Gabrielli, 2011). Nevertheless, there are inequalities in access to health care for both common and rare medical specialties. In particular, rural regions with a low population density, but also certain economically deprived urban areas, combine remoteness of both primary care and specialists (Bagein et al., 2022).
There is no systematic collection of waiting times for access to primary and specialist care in France. While there are a few surveys to estimate access times in ambulatory settings, there is no information on waiting times for surgery for different health problems (such as orthopaedic or cancer surgery). The most recent data, from the 2016 Commonwealth Fund international survey carried out in the general population, suggest that the accessibility of ambulatory care varies according to the type of care needed (Commonwealth Fund, 2016). The share of the French adult population who did not get a same day or next day appointment with their regular physician last time they needed care was 44%, which is much higher than in the Kingdom of the Netherlands (19%), New Zealand (22%) or Australia (31%), even if most EU countries had rates above 40%. Moreover, the share of adults having difficulties in getting after-hours care without going to an ED in France is 64%. In contrast, France was among the countries with the lowest percentage of the population needing to wait two months or more for a specialist appointment (4%, with only Germany presenting a lower rate of 3%) (Commonwealth Fund, 2016). However, data from a national survey carried out in 2016/2017 suggest that waiting times can be longer for certain specialists: the average waiting time for an appointment was 44 days for gynaecologists, 50 days for cardiologists and 80 days for ophthalmologists (Millien, Chaput & Cavillon, 2018).
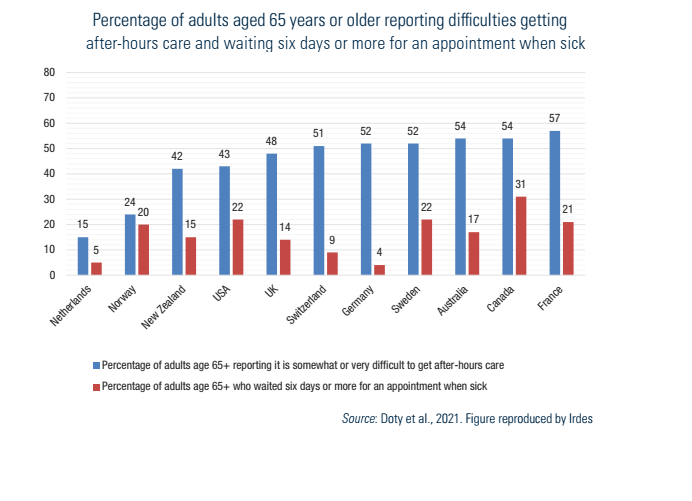
A more recent Commonwealth Fund survey on older adults (over 65 years old) in 2021 confirms that timely access to primary care has not improved over time and can be a problem for vulnerable/older adults. Older people in France had one of the longest waiting times for a general doctor appointment and the highest difficulties in getting after-hours care without going to an ED (Doty et al., 2021) (see Fig7.1). In 2013 it was also estimated that a fifth of 75-year-olds used emergency services for non-urgent care due to a lack of alternative after-hours care (Naouri et al., 2020).
Fig7.1
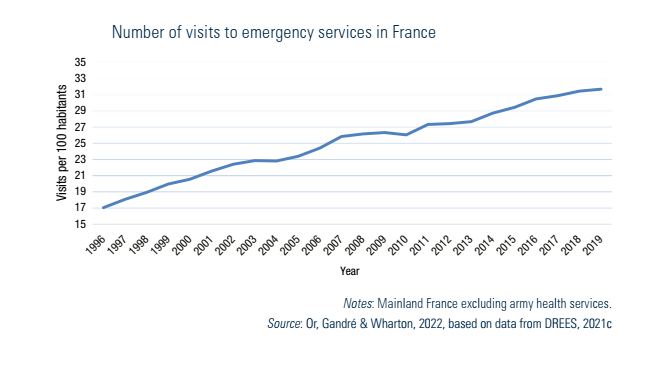
Despite additional payments for MSPs in primary care to extend opening hours, the number of ED visits per capita has almost doubled since 2000, reaching 32 per 100 inhabitants in 2019 (see Fig5.2). In the summer of 2022 exceptional policy measures were introduced to alleviate the pressure on EDs. These included information campaigns for encouraging people to contact first the emergency telephone number (for better triage of patients), higher consultation fees for GPs accepting less severe patients sent by this number, simplifying the recruitment of retired and self-employed physicians in hospitals, and better funding of extra hours (French Government, 2022). These short-term exceptional measures were maintained in the autumn of 2022, and following a positive assessment by the IGAS they will be generalized.
Fig5.2
7.2.3. Unmet care needs
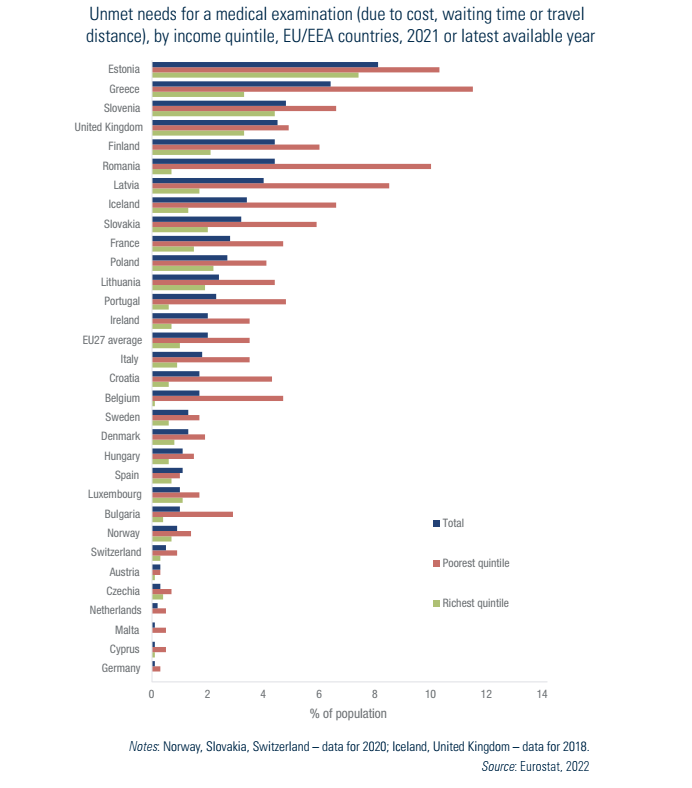
The level of estimated unmet care needs for medical examinations (due to cost, waiting time or travel distance) in 2021 was slightly higher in France (2.8%) compared to the EU average of 2% (Fig7.2). This may be partly due to the restrictions over the period 2020–2021 to contain the spread of the Covid-19 pandemic, which also increased the pressure on the health care system, as well as to inequalities in geographical access to care. Moreover, France has one of the highest income inequalities in unmet care needs: 4.7% of individuals in the poorest income quintiles reported unmet medical care needs compared to 1.5% of those in the highest income quintile in 2021 (vs 3.5% and 1% respectively in the EU overall) (Fig7.2). Despite the mechanisms in place to protect populations with low income and high care needs (see section 3.3.1), there are significant and persisting socioeconomic differences in unmet care needs in France. In 2018 the proportion of unmet dental care needs was 6.7% in the lowest income groups (vs 6.0% in the EU on average) compared to 1.0% in the highest income groups (vs 0.8% in the EU on average) (OECD, 2020c). Since then, France has made progress in increasing the financial accessibility for a selection of dental treatments (see section 7.3) (MoH, 2021a).
Fig7.2
About 18% (approximately 1 million) of surgeries were postponed in 2020 during the Covid-19 pandemic. While the delays were nearly caught up, the volume of surgical procedures was still 5.5% lower than expected at the end of 2021, a rate which varied by specialty and region (CNAM, 2022a). For example, the delays caused by the first lockdown were largely reduced for breast cancer screening and surgery by the end of 2021 thanks to a higher annual activity in the second semester. However, colorectal cancer screening and treatment had not reached their pre-pandemic levels at the end of 2021 (CNAM, 2022a). In addition, more than 35% of LTC recipients at home reported forgone or postponed care during the Covid-19 crisis, which was one of the highest percentages among OECD countries (OECD, 2021d). On a positive note, the deficiencies in care organization at the beginning of the pandemic were addressed over time with, for instance, e-Health solutions to increase the capacity of the health system (Webb et al., 2020). Well-defined care pathways in hospitals for Covid-19 patients allowed for a reduction in pressure on other services and gave space for patients with other conditions (MoH, 2020b). GPs adapted their working practices, and teleconsultations were rapidly expanded to improve access to all care providers (CNAM, 2020g, 2020h).