In the United States there is much interest in maximizing the value of health care services. As discussed earlier in the chapter and throughout the book, a number of health processes in the United States are flawed and health outcomes are often low. At the same time expenditures are extremely high in comparison with other countries. On a number of measures, the United States does not compare well to many other high-income countries, which continue to have much lower expenditures, universal access and oftentimes better measures of quality. Moreover, there is considerable socioeconomic and geographical variation within the United States on these criteria.
Allocative efficiency relates to whether a society’s resources are being spent in the manner that is most beneficial to that society. Relating this to health care, a health care system is operating efficiently if its resources are being spent in a way that best benefits the overall health and well-being of the population. No health care system, of course, operates efficiently by this definition, but a goal of public policy should be to move towards this ideal.
Allocative efficiency comprises three elements. One is technical efficiency, which is discussed below. The second element is whether the right goods and services are being produced. Technically efficient production of the wrong goods obviously falls short of allocative efficiency. The third element concerns how the goods that are produced are distributed.
The second and third elements of allocative efficiency are discussed here, beginning with whether the right goods and services are being produced. Issues include site of services (e.g. inpatient vs outpatient), mix of inputs (e.g. equipment vs labour vs drugs), mix of labour (e.g. specialist physicians vs primary care vs nurses vs psychologists) and mix of services.
Assessing whether the United States is using the “right” mix is extremely difficult. Compared to other countries, the United States uses inpatient care less often; is highly capital and technology-intensive; appears to employ specialists to a somewhat greater extent; and has a mix of services oriented in many ways less towards health promotion and more towards intensive treatment of illness and end-of-life care. To assess allocative efficiency in this regard, it is necessary to examine population preferences, but it is difficult to find reliable sources that examine these issues. Moreover, such data would need to be interpreted very carefully since, as stated in the case of soliciting Americans’ views on national health insurance, “polling questions tend to disguise the more complex reality of the situation” (Blendon et al., 2006, p. 640).
The third part of allocative efficiency concerns whether health care goods and services are being distributed in a way that is consistent with the health needs and tastes of the population. Here it is useful to distinguish between issues of efficiency (the focus here) and those related to equity (discussed in section 7.2). It is nearly impossible to make definitive statements, however, about the desires of the population with regard to health policy. This is illustrated by the fact that since the ACA’s passage 10 years ago, the population has continued to be split over whether they favour or oppose the Act (Kaiser Family Foundation, 2019f). A majority of Americans say they would like to see “Medicare-for-all, in which all Americans would get their insurance from a single government plan” (Kaiser Family Foundation, 2019g). However, people tend to respond less favourably to such questions when told they have to pay more in taxes (Kaiser Family Foundation, 2020c).
Equity and distributional issues have been discussed throughout this chapter as well as in the other parts of this book. Briefly, most of the concerns are related to disparities in access to insurance and care, as well as differences in health care processes and outcomes according to socioeconomic characteristics. In section 7.2 it was shown (among other things) that those with low incomes and individuals and families of Latino origin are far more likely to lack health insurance, the consequence of which is lower use of services due to cost impediments and lack of access to a regular provider of care. The last of these produces its own deleterious consequences, including lack of receipt of many preventive services and initial treatment of chronic diseases such as cancer at a later stage. It was also shown that African Americans have much poorer outcomes than Whites in indicators such as infant mortality, cancer survival and diabetes.
It is beyond the scope of this book to examine the precise relationships between inputs and outputs in the production of health services. Instead, the focus here is on one aspect of technical efficiency: the extent to which health care spending is directed at patient care rather than administration. Everything else being equal, a health care system is operating in a more technically efficient manner if resources expended go directly to patient care.
The issue is nuanced, however. Spending, say, by private insurers on activities such as utilization management is usually thought of as an administrative activity in which resources are being diverted from patient care. But insurers and managed care companies argue that these administrative costs cut unnecessary utilization and expenditures. In fact, to implement the ACA it was necessary to determine which of such costs are indeed counted towards patient care, which in itself creates an administrative burden on both the federal government and insurers. The ACA requires that 80 cents (individuals and small groups) or 85 cents (large groups) of each dollar of premiums be returned to policyholders in the form of health services or quality improvement.
Administrative costs are considerably higher in the United States than in other countries. Private insurers usually operate on a for-profit basis and seek returns for investors. They market through advertising, determine whether a person or group should be eligible to purchase private coverage, and process claims. Obtaining payment from insurers – both public and private – often involves considerable administrative effort. Hospitals and physician groups require substantial resources for administration in dealing with multiple private insurers as well as government programmes.
Cutler and colleagues (Cutler & Ly, 2011; Pozen & Cutler, 2011) report the following in comparing administrative costs in the United States vs. Canada.
A study by Papanicolas and colleagues (2018), published in JAMA, compared the “drivers of spending” responsible for the United States being so much higher than in 10 comparable countries. It concluded that the main reasons were higher prices paid for hospitals, physician services and pharmaceutical drugs, as well as high administrative costs. At the same time, it rejected some other explanations such as “underinvestment in social programs, the low primary care/specialist mix, the fee-for-service system encouraging high volumes of care, or defensive medicine leading to overutilization…” (p. 1034).
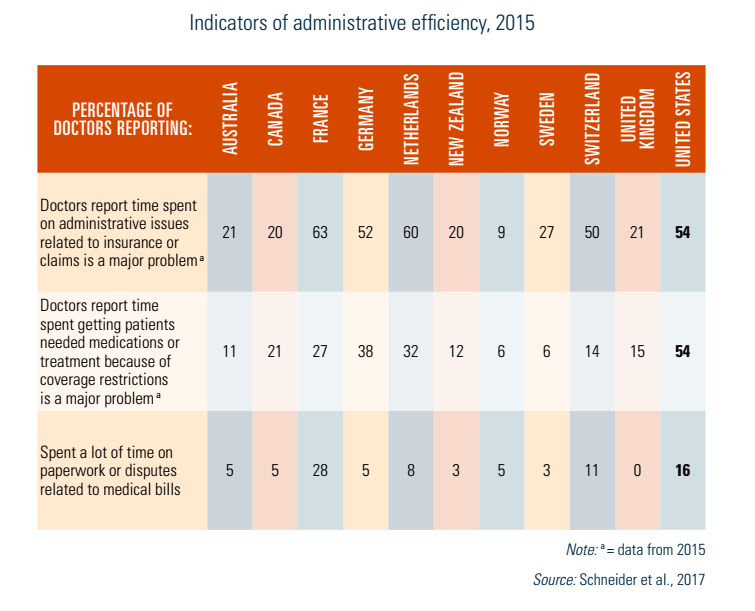
The Commonwealth Fund (2017) study discussed earlier reports on three measures of administrative efficiency among 11 countries. Major problems identified in the report were: (1) time physicians spend on administrative issues related to insurance or claims; (2) time spent on getting patients medications or treatments due to coverage restrictions; and (3) spending a lot of time on paperwork or disputes relating to medical bills. The results are shown in Table7.10. The United States was among the three countries where doctors reported these problems most commonly (along with France and the Netherlands), and had by far the greatest problems for the second measure. As many as 54% of US physicians reported that time spent on getting patients medications or treatments due to coverage restrictions was a major problem. No other country had a figure higher than 38%.
Table7.10