01 July 2024 | Country Update
Expanding the breadth and scope of statutory coverage24 January 2018 | Policy Analysis
Improving access to sick leave for the insured looking after a sick childContext
Until December 2017, insured individuals were entitled up to 45 days of sick leave per year to look after a sick child of up to seven years old (or up to 18 years old for a handicapped child). In cases of communicable diseases, cancers, orthopaedic cast immobilization, and surgical interventions, the treating physician could grant up to 90 days of sick leave, and leaves longer than 90 days could only be granted by a specialist physician with an approval from the Social Security medical expert. Legislation, however, did not cover cases where the sick child was more than seven years old; situations where persons appointed as legal guardians looked after a sick child; or terms for granting sick leave to a person insured in Romania and seeking to look after a sick child in another EU member state or elsewhere (Government of Romania, 2017a).
Impetus for the reform
The need for a change in legislation was brought to the public attention when a TV presenter looking after her 8-year old sick child in another EU member state had to return to Romania and submit a substantial amount of medical documentation and other paper work in order to be granted sick leave (Știrile PROTV, 2017).The case generated public support to change the legislation.
Given the public pressure, in December 2017, the Government issued an Emergency Ordinance to amend the existing legislation, and in January 2018 the Ministry of Health together with the National Health Insurance Fund (NHIF) signed a common Order regulating its implementation. This was in line with the Government Programme 2017-2020, which set out an ambitious vision of “building a balanced society, based on inclusive principles” (Government of Romania, 2017b) by developing citizen-centred health care services (Government of Romania, 2017c).
Content of the reform
The main objective of the reform is to increase access to sick leave by extending coverage and by reducing bureaucracy. The specific measures to increase coverage include: extending the age limit of the sick child with certain severe conditions from 7 to 16 years of age, with both parents and legal guardians being entitled to sick leave to look after the child, as long as they are insured; introducing entitlement to sick leave for those seeking to care for a sick child in another EU member state; providing the possibility of obtaining voluntary sick leave insurance from the NHIF for those who are not insured. Several measures have also been included to simplify the paperwork when requesting a sick leave, in particular: the possibility of having electronic sick leave certificates sent directly from the issuing physician to the employer; the possibility to obtain a sick leave certificate for a child treated in another EU member state within 15 days from the return to Romania; and the possibility of having an authorised person submit required sick leave documentation to the NHIF instead of submitting them in person (Government of Romania, 2017d).
Evaluation
There is no evaluation plan for this specific policy, but it is expected that process and output indicators will be reported in the periodic reports on the Implementation of the 2017-2020 Programme for Government. Further, as the implementation of electronic sick leave certificates is also a performance indicator of the National Public Health Strategy, an assessment is expected. An evaluation using surveys of patient satisfaction in the medium term may capture the success of this legislative change.
Government of Romania (2017a). Notă de fundamentare la Ordonanţa de urgență a Guvernului nr. 99/2017 pentru modificarea şi completarea Ordonanţei de urgenţă a Guvernului nr. 158/2005 privind concediile şi indemnizaţiile de asigurări sociale de sănătate [Substantiation note to the Emergency Ordinance of the Government no. 99/2017 for the amendment and completion of the Emergency Ordinance of the Government no. 158/2005 regarding the sick leave and medical allowance] (http://gov.ro/ro/guvernul/procesul-legislativ/note-de-fundamentare/nota-de-fundamentare-oug-nr-99-14-12-2017&page=1, accessed 17 January 2018)
Știrile PROTV (2017). [PROTV News]. Prezentatoarea TV Magda Vasiliu: Fiul meu e tratat de cancer în Italia, iar România, țara mea, îmi cere acte peste acte [TV presenter Magda Vasiliu: My son is treated by cancer in Italy, while Romania, my country, asks for papers] (http://stirileprotv.ro/stiri/actualitate/prezentatoarea-tv-magda-vasiliu-fiul-meu-e-tratat-de-cancer-in-italia-iar-romania-tara-mea-imi-cere-acte-peste-acte.html, accessed 17 January 2018)
Government of Romania (2017b). Programme for Government 2017-2020. Vision (http://gov.ro/en/objectives/programme-for-government-2017-2020, accessed 17 January 2018)
Government of Romania (2017c). Program de guvernare 2017-2020 aprobat prin Hotărârea nr.53 din 29 iunie 2017 a Parlamentului României pentru acordarea încrederii Guvernului, publicată în Monitorul Oficial al României, Partea I, Nr. 496/29.VI.2017 [Programme for Government 2017-2020 approved by the Parliament Decision no. 53/2017 for granting confidence to the Government, published in the Official Gazette of RomaniaPart I, No. 496/29.VI.2017] (http://mrp.gov.ro/web/programul-de-guvernare-2017-2020/, accessed 17 January 2018)
Government of Romania (2017d). Ordonanța de urgență a Guvernului nr. nr. 99/2017 pentru modificarea şi completarea Ordonanţei de urgenţă a Guvernului nr. 158/2005 privind concediile şi indemnizaţiile de asigurări sociale de sănătate [Emergency Ordinance of the Government no. 99/2017 for the amendment and completion of the Emergency Ordinance of the Government no. 158/2005 regarding the sick leave and medical allowance].Monitorul Oficial Nr.1005 din 19 decembrie 2017 [Official Gazette No. 1005 of 19 December 2017] (http://www.casan.ro/casalba/media/postFiles/OUG%2099-mod.%20OUG%20158.2005.pdf, accessed 17 January 2018)
According to the provisions of Law 95/2006, the social health insurance system is compulsory for all citizens, as well as for foreign residents in Romania, and opting out is not possible. The main criterion for entitlement is proof of contribution payment or of status that allows coverage without contribution. When accessing health care services, if not already registered with the SIUI (see section 2.7.1) one must present a certificate of registration from the DHIH. This certificate can be obtained by showing, among others, evidence of payment of insurance contributions for the past five years. Any missing contributions (including penalties) must be paid in order for this certificate to be issued. The National Health Insurance Card, which was introduced in 2015 (see section 4.1.4), should be presented at the point of health service delivery, together with proof of contribution payment or exemption, as a tool that validates service provision in the NHIH’s system and ensures that the provider is reimbursed. It is also seen to prevent fraudulent reporting of health care services; for example, with the electronic system it will be very difficult to report services that were not provided or to issue drug prescriptions to fictive patients.
Other population groups entitled to benefits are: permanent or long-term residents or persons staying temporarily in Romania, foreigners or stateless persons, citizens of EU Member States, EEA states or the Swiss Confederation not insured in other EU Member States; citizens of EU Member States, EEA states or the Swiss Confederation who are cross-border workers working in Romania and reside in other EU Member States, EEA states or the Swiss Confederation; Romanian pensioners who are resident in other EU Member States, EEA states or the Swiss Confederation or in a country with which Romania has a mutual social security agreement with provisions regarding health insurance (see section 2.9.6).
Some population categories are exempted from the contribution payment. Their contributions are paid by one of the following sources: the unemployment insurance budget from the Ministry of Labour, Family, Social Protection and Elderly covers the unemployed; the work accident and occupational disease insurance fund covers persons on sick leave due to a work accident or occupational disease; the state budget covers persons in penitentiaries, persons on maternity leave for up to two years (three years for children with disabilities), pensioners with incomes under 740 lei a month (approximately €155), refugees during the period of status clearance, persons living on social benefits, monks, nuns and other personnel living and working in the monasteries with no income, and so on. The following population groups are insured with no obligation to pay insurance contributions (provision of health care services for these groups is financed from the contributions of the paying population): children and young people up to 26 years old if they are enrolled in any form of education or are coming out from child protection institutions and have no own income; war veterans and their widows; victims of political persecutions between 1945–1989; people with disabilities; chronically ill patients covered under national health programmes; pregnant women (Law 95/2006).
Although social health insurance is compulsory, in 2014 only 86% of the population was covered, with the proportion higher among those living in urban areas, at 94.9%, compared to rural areas at 75.8% (NHIH, 2015a). The uninsured are: people working in agriculture or those not officially employed in the private sector; self-employed or unemployed who are not registered for unemployment or social security benefits; and Roma people who do not have identity cards, which precludes them from enrolling into the social security system. The uninsured can only access a minimum benefits package, which is strictly enforced. This package covers emergency care, treatment of communicable diseases and care during pregnancy.
Some population groups cannot access health care services due to: lack of knowledge regarding the benefits to which they are entitled (see section 2.9.1); lack of respective services in their area of residence (e.g. family medicine physicians in some remote areas) combined with the lack of resources to cover travel costs and/or poor transport infrastructure; and scarcity of financial resources in the health care system. For example, until 2015, patients undergoing hospital treatment could be offered the option of purchasing necessary drugs or materials themselves when the hospital where they were treated was not able to offer them free of charge; this practice has been forbidden since 2015.
The insured population is entitled to a basic benefits package described in the Framework Contract (see section 2.8.1). The basic benefits package is standard across the whole covered population and includes health care services, pharmaceuticals and medical devices. The minimum package for uninsured persons is set on the basis of three main criteria: life-threatening emergencies, epidemic-prone/infectious diseases and birth. Covered health care services include: preventive health care services, ambulatory health care, hospital care, dental services, medical emergency services, medical rehabilitation services, pre-, intra- and post-birth medical assistance, home care nursing, drugs, health care materials and orthopaedic devices. Insured persons are entitled to health care services from the first day of sickness or the date of an accident until they are fully recovered.
The list of excluded services is provided by Law 95/2006, by listing services that are paid by other sources (e.g. services covered by the insurance fund for work accidents and professional diseases), services requiring very expensive technology or services that are considered not to have a medical justification (e.g. plastic surgery for aesthetic corrections, in vitro fertilization (IVF)) (see section 3.4).
The NHIF’s budget also covers cash benefits in case of sickness leave. Cash benefits in other situations (e.g. disability, invalidity, etc.) are paid by other funds of the social security system (see section 2.1). Since 1 January 2007, when Romania joined the EU, the NHIH has provided insured persons (upon request) with the EHIC, which allows them to receive necessary medical assistance during a temporary stay in an EU/EEA country and Switzerland, in accordance with specific EU regulations transposed into the Romanian legislation (see section 2.9.6).
Decisions on the services and goods to be included or excluded from the statutory benefits package are taken by the NHIH and the Ministry of Health. There are no clear inclusion or exclusion criteria and decisions are based on consultations with different actors. For pharmaceuticals, a positive list is elaborated by the NAMMD with input from their newly created HTA department (see section 2.7.2).
Cost-sharing is applied for certain goods and services included in the basic benefits package (see section 3.4). For pharmaceuticals delivered within ambulatory care, patients have to pay 10% of the reference price for generic prescription drugs and 50% for branded or innovative prescription drugs. For expensive prescription drugs, with prices higher than the reference price, a patient’s contribution can be as high as 80% of the retail price. The aim of having user charges (co-plata in Romanian) is to control the costs of prescription drugs. Cost-sharing is also applied to balneary (spa) treatment and rehabilitation services. The patient pays 30–35% of the daily tariff and pays the full tariff for lengths of stay over 14–21 days and for non-emergency admissions without a referral. From 2013, hospitals have also been charging a small co-payment for hospital admissions (less than €2.5, payable at discharge), with the aims of reducing hospital admissions and increasing the income of hospitals. The following groups are exempted from hospital co-payment: children and young adults up to 18 years old and young people up to 26 years old if they are enrolled in any form of education; patients covered by the national health programmes; pregnant women without income; and pensioners with income under 740 lei (approximately €155) per month. The impact of this new user charge has not been evaluated but so far appears to be marginal.
The DHIHs can sign contracts for health care provision with private providers. The amount of reimbursement these providers receive is the same as public providers but, unlike public providers, they can charge, on top of the amount reimbursed, an additional fee for the services they provide (extra billing). This applies only to secondary health care (ambulatory and inpatient) and not to primary health care.
In 2023, the low share of the population covered by statutory health insurance (around 87% in 2019) led to the decision to extend the benefits package of primary healthcare services to the uninsured population. Uninsured patients still had to pay out of pocket for the lab tests and imaging investigations then, as well as for the outpatient medicines prescribed by a family doctor.
From 1 July 2024, the benefits package was further adjusted to include services for uninsured populations that will ensure early detection and early treatment for several serious diseases such as cancers, hepatitis B and C, and HIV/AIDS in pregnant women.
In particular, the new services covered for uninsured people include: lab tests and specialist visits for uninsured patients suspected to have any type of cancer; testing for hepatitis B and C; and testing for HIV/AIDS for uninsured pregnant women. These services will be reimbursed to laboratories, ambulatory services and hospitals (day hospitalization) for these patients once the diagnostic is confirmed. These services will also be provided by and reimbursed to mobile healthcare units, to increase access for populations in remote, isolated areas.
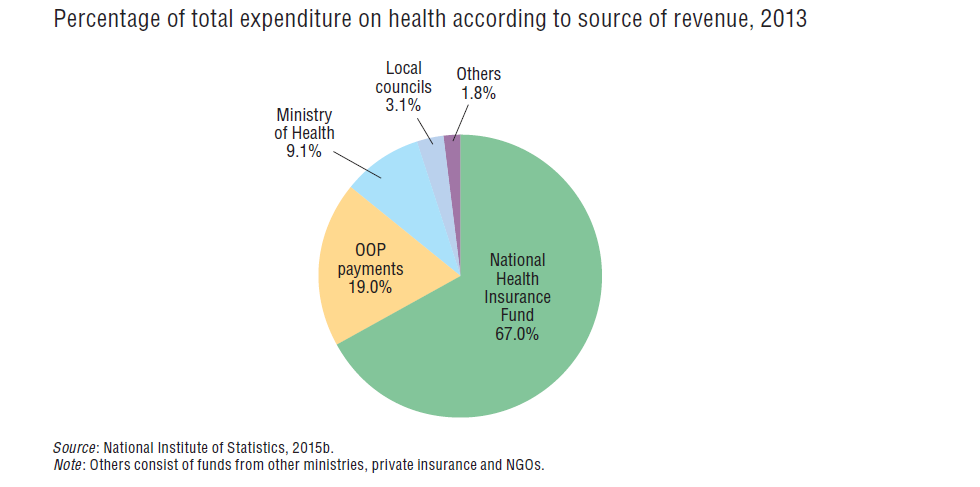
In 2013, state (Ministry of Health) and local budgets accounted for about 12% of total health financing (see Fig3.5). This revenue comes from taxation and does not include funds from other budgets such as insurance contributions for exempted population groups (this is included in the NHIF’s income). Taxes are not specifically earmarked for health, except for some special taxes imposed on tobacco and alcohol production, import and procurement, with the purpose of controlling their consumption.
Fig3.5
The overall tax-to-GDP ratio of Romania is one of the lowest in the EU, at 28.3% in 2012, compared to an EU GDP-weighted average of 39.4%. Romania has the second highest reliance on indirect taxes in the EU. In 2012, indirect taxes accounted for 47.2% of total tax revenue compared with 34.5% for the EU average, while the share of social insurance contributions accounted for 31.2% (32.4% in the EU) and direct taxes for only 21.6% (33.4% in the EU) (Eurostat, 2014).
The individual and corporate income tax rates for 2015 were flat at 16%. Capital gains of companies and individuals were also taxed at 16%. For individuals the tax rate for gain from sale of real estate is 1–3%. Besides general and local taxes and social health insurance contributions (see ‘Contributions pooled by the NHIF’ below), employers and employees contribute to the social security fund, with 15.8% paid by employers and 10.5% by employees, and the unemployment fund, at 0.5% each. In addition, employers must pay a number of other contributions, e.g. for disability (www.worldwide-tax.com, 2015).
The Ministry of Public Finances, through its structures, is responsible for collecting both general and local taxes,[5] and contributions for specific funds. The NHIF’s annual budget is proposed by the government and approved by the parliament as an annex in the Budget State Law (see section 3.3.3). Contributions are collected at the central level by the National Agency for Fiscal Administration. Taxes, through different budgets (state budget, social insurance budget, unemployment insurance budget and local budgets) also cover insurance contributions for some population categories exempted from the contribution payment (i.e. people during military service or detention, medical leave, the unemployed, people under social security benefits schemes, etc.). The collection rate for social health insurance contributions is not 100%, as some entities do not pay the full amount due.
Revenue of the NHIF comes from contributions paid by the insured population and employers, state budget subventions and transfers, and other sources (donations, interest rates, etc.) (see section 3.3.1). In 2014, the structure of the NHIF’s income was as follows: 76.3% from contributions (36% from employers, 40.3% from insured persons); 16.8% from the state budget, including subventions from the state budget; 6.6% from the claw-back tax; and 0.3% from other sources (NHIH, 2015a).
Contributions are collected by the National Agency for Fiscal Administration, under the remit of the Ministry of Public Finances. Since the social health insurance scheme is compulsory by law, those who cannot provide a proof of being insured when accessing health care services may be liable to pay the legal contributions (and penalties) retrospectively (for up to six months, unless they can prove they had paid the contributions in some of those months).
Contribution rates vary for the insured population and employers. The contribution rates are set by Law 95/2006. The rates in 2014–2015 were: 5.5% of gross salary from the insured and 5.2% from the employer. In 1999, the rate was 7% (uniform for both employees and employers). The self-employed pay 10.7%. The contribution paid by the insured is calculated on gross income obtained from salaries, independent activities, agriculture, lettings, pensions (income over the tax base limit, which is 740 lei or €155 per month), dividends and interests on personal bank reserve accounts.
Some population categories are exempted from the contribution payment, either with the contributions paid on their behalf (e.g. from the unemployment insurance budget for the unemployed) or with no payment obligation (see section 3.3.1). Between 2002 and 2004 exemption from the contribution payment was extended to cover more population groups (e.g. pensioners and beneficiaries of social security benefits) so that, by 2005, only 5 million people were paying insurance contributions, while 22 million were entitled to benefits (Scîntee & Vlădescu, 2006). This was changed by Law 95/2006 and subsequent amendments, which reduced the number of exemptions; for example, pensioners whose income (pension) is over the taxation base have been required to contribute since 2010, with contributions due only on the amount that exceeds the taxation base or on other extra-pension incomes.
The overall health care budget, including the budget of the NHIF, is set annually by the government and approved by the parliament through the State Budget Law. The majority of the health budget (61%) is allocated through the Ministry of Health, 33% via local budgets and 6% through other ministries (2013) (National Institute of Statistics, 2015b). Some of the budget can also be transferred to the NHIF to pay for drugs and treatments or added to the Ministry of Health’s reserve (Law 95/2006). State funding for health is earmarked for specific purposes before distribution to the Ministry of Health and to the other ministries with their own health networks. Funds that are allocated to one spending category cannot be transferred to another. The Ministry of Health allocates funds to the DPHAs or directly to its subordinated units (i.e. hospitals, institutes of public health) in accordance with the approved budget. Allocations to the DPHAs are based on proposals made by the representatives of the DPHAs and rely heavily on historical allocations. Funds allocated to the preventive national health programmes are distributed to different institutions according to their responsibilities in programme implementation. Budgets for capital investments (see section 2.8.6) are included in the annual programmes developed by the Ministry of Health and are based on a specific methodology. The programmes are included as an annex in the State Budget Law. Funds for capital investments are transferred from local budgets to health care facilities on the basis of a pre-approved capital investment plan (see Vlădescu et al., 2008b).
The funds for services under the social health insurance system are pooled in the NHIF. These funds include: contributions collected by the Ministry of Public Finances through the National Agency for Fiscal Administration; contributions paid from different public budgets for certain categories of the insured; transfers from the Ministry of Health for treatments under the national health programmes; and other incomes. According to the law, in justified situations, the NHIF’s deficit can be covered by subventions from the Ministry of Health budget, after the NHIF’s reserve fund is exhausted (Law 95/2006). The NHIF is administered by the NHIH that allocates money to the DHIHs for purchasing services, in accordance with the approved budget. As with the DPHAs, the allocations are based on the proposals of the representatives of the DHIHs and rely on historical allocations. One per cent of the total annual NHIF budget is retained as a reserve. This reserve fund can only be used if there is a budget surplus and only after all outstanding debts have been paid (Law 95/2006).
The DHIHs purchase services on behalf of the insured population in their respective geographical areas. Each DHIH receives a budget from the NHIH. The budget determines the allocation for each type of health service the DHIHs have to purchase. No adjustment is allowed at the purchaser level (except for when reserve funds can be used, in which case the allocation can be increased; see above).
All purchasing contracts concluded between the DHIHs and providers must comply with the Framework Contract and its implementation norms (see section 2.8.1). The implementation of the Framework Contract is monitored by special departments at both the NHIH and DHIH levels. Other departments in these institutions periodically monitor providers in order to check compliance with the contract for provision of services; compliance checks are undertaken for volume but, although there are provisions for monitoring quality, this is not implemented in practice, due to lack of capacity (see section 2.8.2). The Framework Contract sets the sanctions for each type of violation or failure to meet the obligations under the contract. Sanctions are foreseen for both the DHIHs and service providers. The same contracting rules apply to both public and private providers. There is no competition and the DHIHs usually sign contracts with all providers in the district (see Vlădescu et al., 2008b).