Mental health care is growing in importance and in 2015 (latest available year) 13% of total health expenditure was spent on mental health care, which is the third highest spend per disease entity in Germany (Statistisches Bundesamt, 2017).[18] Beyond directly related health expenditure, mental health is also a main driver for indirect health expenditure such as (long-term) leave due to incapacity to work (23.1% in 2014). Depressive episodes, in women and men alike, were the most often reported cause of incapacity to work and caused roughly a fourth of related costs in 2014 (Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen, 2015). More recent analysis has reaffirmed an increase in mental health-related utilization of health services and costs (BARMER Institut für Gesundheitssystemforschung, 2020).
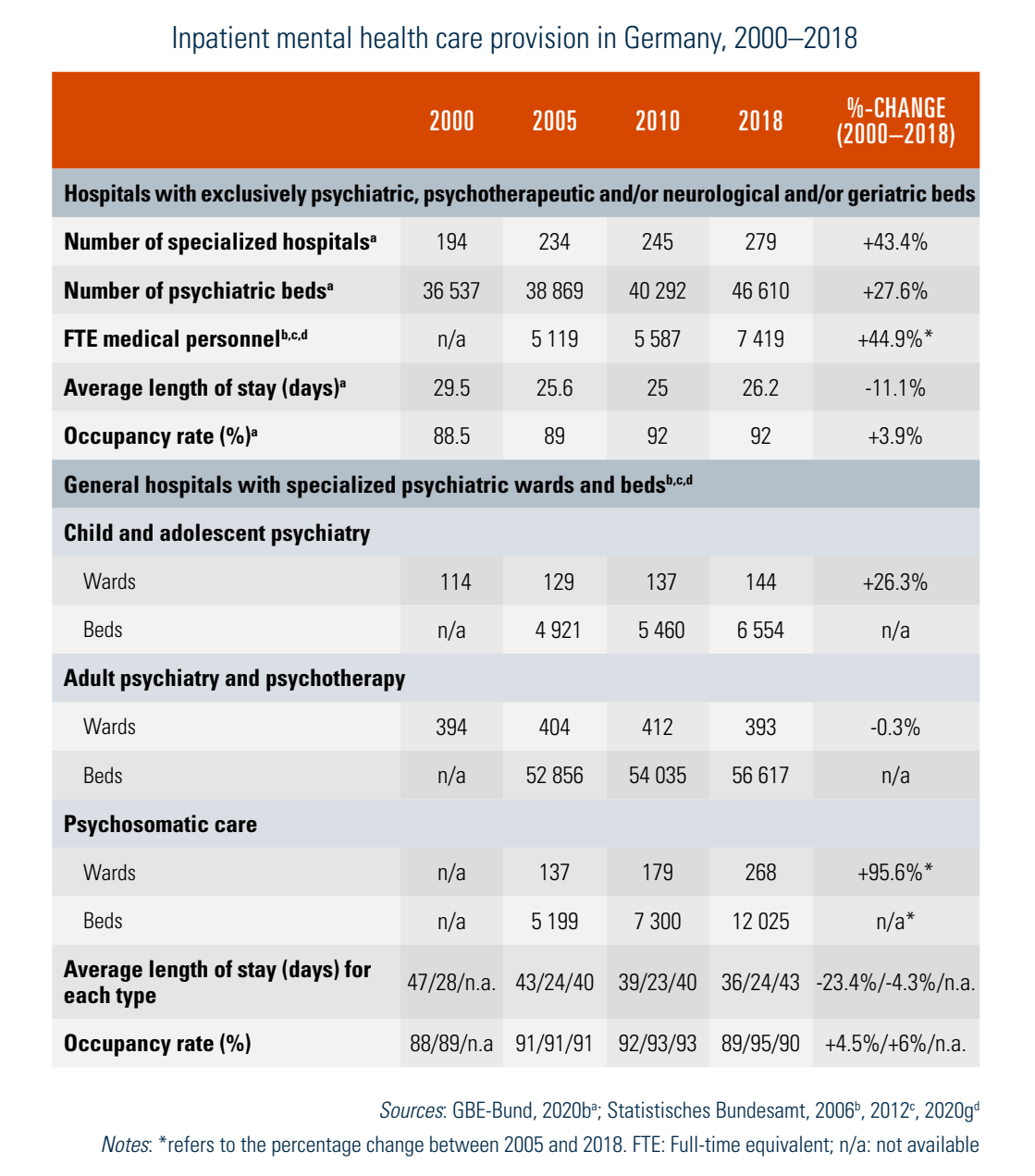
Provision of mental health care is fragmented among ambulatory, inpatient and rehabilitative care. These services are complemented by an integrative service for disabled persons, preventive services and patient groups. After a process of deinstitutionalization that started in the mid-1970s, since the year 2000 there has been an increase in capacity through specialized hospitals and in general hospitals with specialized mental health wards. Simultaneously, the average length of stay has been reduced to 26.2 days in 2018. Characteristically, all inpatient psychiatric care units have very high occupancy rates of around or above 90% (Table5.4). In 2018 there were 279 specialized hospitals solely dedicated to psychiatric care, with a total of 46 610 beds. In addition, there were 805 psychiatric wards in acute care hospitals with a total of 75 196 beds; of these, 144 wards specialized in child and adolescent psychiatry (6554 beds).
Table5.4
In 2018 a total of 891 711 patients were treated in inpatient psychiatric care (specialized hospitals and psychiatric wards combined; equal to 1069 diagnoses per 100 000 population). The treatment of depressive episodes was responsible for a fifth of all psychiatric hospital stays in 2018. Since 2018 psychiatric hospitals have been reimbursed based on clinically defined groups with comparable costs (Pauschalierendes Entgeltsystem Psychiatrie und Psychosomatik – PEPP), which also allows for a more detailed analysis of inpatient psychiatric care (GBE-Bund, 2020b).
Like general inpatient care, the states are responsible for planning of inpatient psychiatric care. They detail the number and setting of beds in hospitals (and also decide on designated specialized psychiatric hospitals or whether to shift provision to general acute hospitals) (AG Psychiatrie der AOLG, 2007, 2017). Psychiatric outpatient departments (Psychiatrische Institutsambulanzen – PIA) are another means of providing mental health care. These services are based at psychiatric hospitals which have been authorized by the Accreditation Committee to provide outpatient psychiatric and psychotherapeutic care for insured individuals.
The process of deinstitutionalization was accompanied by an increase in the number of community-based institutions, especially supervised residential arrangements, ambulatory crisis intervention centres, and centres for psychosocial counselling and social support. These are frequently run on a not-for-profit basis. At the same time, there was an increase in the number of hospitals (and beds) dedicated to prevention and rehabilitative care that lie outside the state hospital requirement plans. Often owned by private for-profit providers, these institutions specialize particularly in caring for patients with addiction problems and psychosomatic conditions. Ambulatory care for the mentally ill patients (adults and children) is supported by the increasing number of office-based psychiatrists, neurologists and psychotherapists working in the ambulatory care sector (see section 5.3 Primary care). In 2018 there were approximately 46 000 psychotherapists (including child and youth psychotherapists), most of them employed in the ambulatory care sector (34 000 or 73.9%) (Statistisches Bundesamt, 2020e). The number of these medical professions has increased over the last few years, with psychotherapists recording a five-year increase of 32% since 2014 (Kassenärztliche Bundesvereinigung (KBV), 2014, 2019d).
Planning of providers and services covered under SHI is the responsibility of the Federal Joint Committee and the Regional Associations of SHI Physicians respectively. Since 2000 ambulatory psychiatrists have been made coordinators of a set of benefits called “sociotherapeutic care” to encourage people with chronic mental health conditions to utilize necessary care and to avoid unnecessary hospitalizations. In 2017 a directive of the Federal Joint Committee further regulated psychotherapeutic counselling, which is conceptualized as the first contact point for ambulatory psychotherapeutic services. Psychotherapists have to reserve at least 100 minutes a week for these psychotherapeutic counselling sessions (in person for at least 25 minutes, also possible as group sessions). If there is an acute need for treatment, an acute psychotherapeutic treatment can follow to help the patient cope with their personal crisis and avoid hospitalization (the line of treatment is capped at 24 interventions of 25 minutes). In addition, and if there is free capacity in terms of therapy places, long-term psychotherapeutic treatment can follow these options. The 2017 directive also introduced a form of prevention for recurring episodes through follow-up sessions after a psychotherapeutic treatment (Gemeinsamer Bundesausschuss, 22.09.2019).
In the past, the availability of ambulatory psychotherapeutic care was perceived as a key problem with long (and regionally diverse) waiting times for a therapy place. This was targeted in 2015 by the Healthcare Strengthening Act by installing central service points for booking appointments at each of the Regional Associations of SHI Physicians. In 2018 a representative study among those insured by one of the largest sickness funds indicated that 90% of those insured wishing to book an appointment directly approached private practices, and 8% used a central service point. Some 80% reported being able to book an appointment within four weeks with a psychotherapist (BARMER Institut für Gesundheitssystemforschung, 2020). Another study indicated an average waiting time of 5.7 weeks for a counselling session in 2017. However, there are regional differences: in urban regions such as Berlin waiting times of 3.4 weeks were recorded, compared to a maximum of 11 weeks in rural areas (Bundespsychotherapeutenkammer (BPtK), 2018). Both studies report that roughly 10% of contacts had no need for a psychotherapeutic treatment and 20% were directed to other forms of counselling, such as patient groups. However, there are still waiting times for (long-term) therapy places of around five months.
The quantity, comprehensiveness and quality of ambulatory psychotherapeutic services vary largely between different local communities and states. Despite advances, psychosocial facilities are often less well equipped than institutions for somatic care, and access to occupational rehabilitation and comprehensive social integration is still considered insufficiently developed. Additionally, public health offices provide social-psychiatric services, including counselling, social work, home visits and crisis intervention, directed particularly at the most disadvantaged among the mentally ill.