At the end of 2011, there were 2694 hospitals in France. Non-profit-making institutions accounted for 61% (35% public and 26% private sector) and 39% were private hospitals operated for profit (DREES, 2013c).
The 947 public hospitals account for nearly two-thirds of inpatient beds (258 156 out of 414 395). There are three main types of public hospitals:
There are also 24 other public establishments, primarily imaging and radiotherapy centres.
Private hospitals fall into two categories: non-profit-making or profit-making. Non-profit-making hospitals are owned by foundations, religious organizations or mutual insurance associations. In 2011, they accounted for 26% of hospitals (700) and 14% of inpatient beds (11 778). Two-thirds of private non-profit-making hospitals perform public service duties such as emergency care, teaching and social programmes for deprived populations; they are known as “participants in public hospital service” (participant au service public hospitalier). Nineteen of them specialize in cancer treatment, with a broad remit that includes prevention, screening, treatment, teaching and research.
The private profit-making sector plays an important role in the French health care system. The share of hospitals that are operated for profit is higher than in most developed countries: private profit-making hospitals accounted for 39% of all hospitals (1047) and 24% of all inpatient beds (98 522) in 2011. They also accounted for 22% of part-time hospitalization places and tend to specialize in areas with higher profit opportunities (see section 5.4).
The market for hospital care is becoming increasingly concentrated. The number of hospitals has been declining since 1990, mainly because of hospital closures and mergers within the private sector. Nonetheless, new modes of cooperation may result in an increase in the number of hospitals over the next few years.
The overall area of the property assets of public hospitals is estimated at 60 million square metres, a scale comparable to the rest of the state’s property holdings. However, to date, record keeping has not been standardized among hospitals, and consequently the ministry in charge of health has lacked reliable data in this regard (Cour des comptes, 2013a). In 2014, a new tool called OPHELIE was launched to remedy this problem by standardizing the inventory control and facilitating management of hospital property assets. Focusing initially on hospitals with investment projects, those undergoing audits as well as hospitals volunteering to participate, it will be rolled out to all public hospitals by 2017.
Depending on the specific sector and public health priorities, capital investments in the health care sector are either covered by reimbursements for service delivery or funded by specific national or regional programmes. Between 1983 and 2003, the public and private non-profit-making sectors suffered from a lack of investment because of the financial constraints imposed by the global budget payment system in place at that time. Since then, two nationwide investment programmes have been launched to support improvements to meet current quality and safety standards: Hospital Plan 2007 (Plan Hôpital 2007) and Hospital Plan 2012 (Plan Hôpital 2012).
Hospital Plan 2007 was launched in 2003 as part of an ambitious reform of the hospital sector; €6 billion was invested over five years for select projects proposed by public and private hospitals. The plan was to be entirely funded by SHI, in part by direct funding of the investments (€1.5 billion) and in part by underwriting 20-year loans to the hospitals (€4.5 billion). The Hospital Plan 2007 also provided for public–private partnerships (partenariat public–privé), and each of the regional hospital agencies (Agences régionale de l’hospitalisation, predecessors to the ARSs) was to propose at least one public–private partnership investment project. The French Accounts Commission (Cour des comptes) criticized the realization of these partnerships as being insufficiently planned and executed (Cour des comptes, 2014a). Since 2012, national oversight of investments undertaken by the ARSs and valued at over €50 million has been provided by the Interministerial Committee for Performance and Modernization of the Health Care Supply (Comité interministériel de performance et de la modernisation de l’offre de soins).
The second investment plan, Hospital Plan 2012, was introduced in 2007 in order to extend the previous investment cycle. This new plan involved an initial endowment of €7 billion, again financed by SHI through direct funding (€5 billion) and through access to public lending at preferential interest rates (€2 billion). This plan has three major priorities: hospital information technology systems, restructuring of hospital facilities at the regional level (e.g. collaborations and mergers between hospitals) and improvement of compliance with safety standards (e.g. seismic compliance and asbestos removal).
In 2013, the strategy to support investment in health was reinforced with the goals of ensuring that investments were aligned with patient pathways, that they conformed to the strictest standards, that they integrated digital programmes and that they ensure financial sustainability. Regional schemes for investment in health (schémas régionaux de l’investissement en santé) were put into place in 2013, with the objective of ensuring coherence of investments at the regional level. Part of the focus of the regional schemes involves examining investments undertaken within the previous 10 years and identifying existing capacity available to meet the needs identified by the ARSs. This effort will be aided by the data compiled by the OPHELIE tool, which will enable consideration of future investment projects in light of existing property assets.
In December 2013, the French Government signed an accord with the European Investment Bank, which will finance public and private hospital construction and renovation projects under the Hospital of the Future Programme, amounting to €1.5 billion over three years.
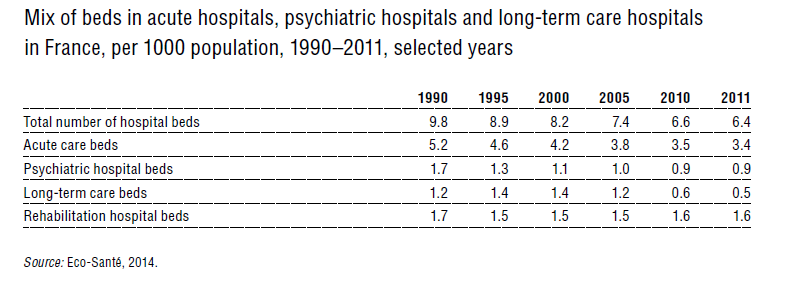
In 2011, France had an average of 6.3 full-time hospital beds and 1 part-time hospital bed [3] (referred to as places) per 1000 inhabitants, with more than half the beds and 42% of the places dedicated to acute care (Table4.1). In addition, 0.02 places per 1000 inhabitants were available for home hospitalization services, 97.6% of which were dedicated to acute care.
Table4.1
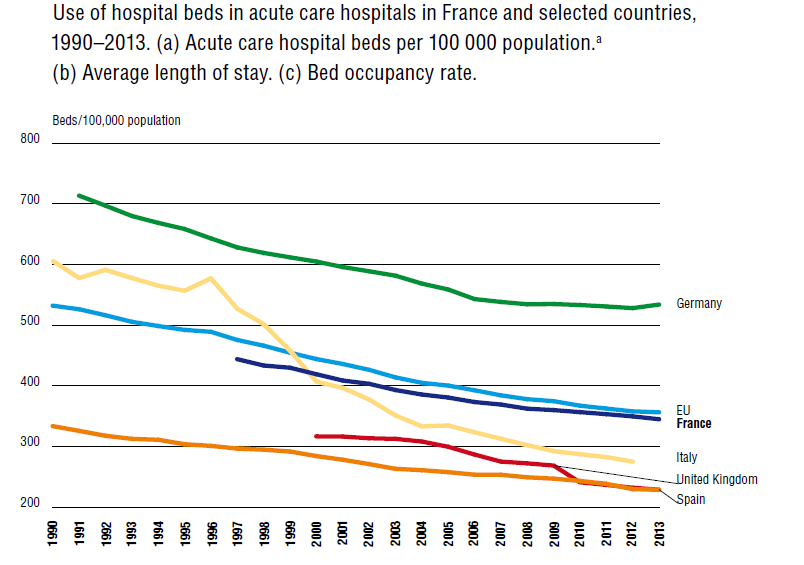
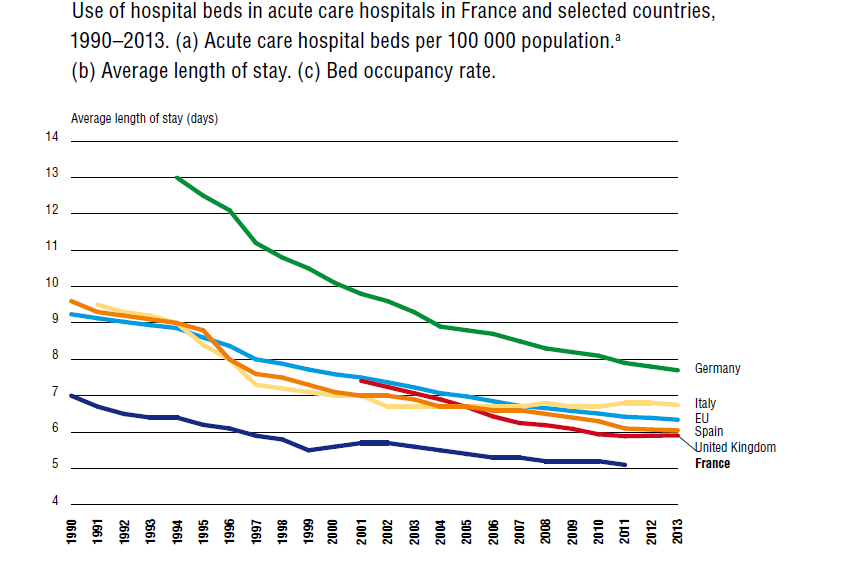
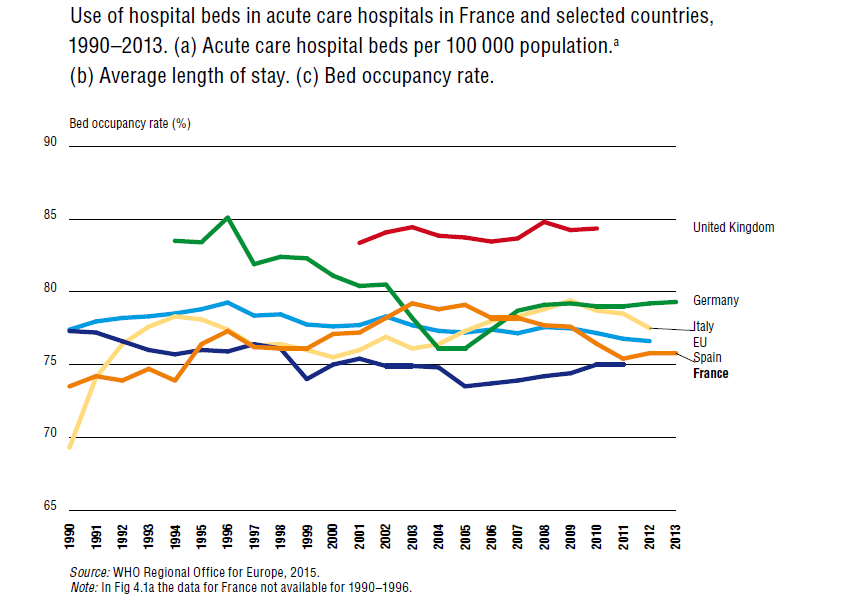
Consistent with the general trend among European countries, the total number of hospital beds in France has declined since 1990. Between 2003 and 2011, the number of full-time hospital beds fell from 468 000 to 414 000. The number of acute care beds has been steadily declining since the late 1980s (Fig4.1a). Average length of stay in acute hospitals also has diminished, being lower than in comparable European countries, with an average length of stay of five days in 2011 (Fig4.1b). Bed occupancy rates have remained fairly stable (Fig4.1c).
| Fig4.1a | Fig4.1b | Fig4.1c |
 |  |  |
The reduction in hospital capacity was most significant with respect to long-term care beds, which decreased by 40% between 2003 and 2011 through the transformation of certain units into nursing homes. Full-time psychiatric hospitalization capacity has also diminished significantly since the mid-1980s as a result of the French deinstitutionalization policy (see section 5.11), accounting for approximately 58 000 hospital beds in 2011. Between 2003 and 2011, the number of part-time places increased by 2000, reaching 14 243.
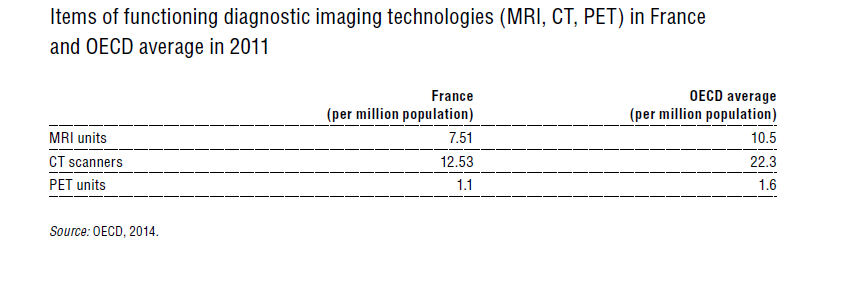
Purchase of major medical equipment is subject to authorization by the relevant ARS (see section 2.8.6). Two-thirds of CT and MRI units are found in public hospitals, although the number of MRI units is rapidly growing in private hospitals because of advantageous SHI tariffs. PET scanners are less profitable and so are less likely to be found in private hospitals. In 2011, the number of major medical imaging technologies was lower relative to population size than the OECD average (Table4.2). The availability of MRI units, in particular, has been questioned, in terms of both waiting times and geographic dispersion (Cour des comptes, 2010).
Table4.2
In France, the development of the Internet has been rather slow compared with other European countries but has improved in recent years. By June 2012, 81% of people aged 12 years or over had access to the Internet at home, reflecting a 3% increase over 12 months (CREDOC, 2012). In addition, the Internet was often used for health-related purposes: in the same study, 37% of French population reported having looked for health information for themselves or one of their relatives on the Internet (Bigot & Croutte, 2011). The government has taken the initiative in establishing health care information websites for the general public, including a searchable drug database (Base de données publique des médicaments; http://base-donnees-publique.medicaments.gouv.fr) and Scope Santé (http://www.scopesante.fr), which provides information on hospital quality indicators.
Since the late 1980s, the French health care sector has seen a slow but continuous development of its information technology infrastructure (see section 2.7.1). Recently, development of information technology systems has become a priority on the political agenda, mainly because it is seen as a way to improve the efficiency of the sector. Moreover, in its 2013 National Health Strategy, the government underscored the need to ensure compatibility and interoperability among the information technology systems in the ambulatory, hospital and medicosocial sectors (Ministry in charge of Health, 2013).
Data from the PMSI (see section 2.7.1), which was first developed in the 1980s and became exhaustive with respect to acute care in 1996, formed the backbone of the T2A (see section 3.7.2), which has been in use since 2004.
An electronic billing system has been gradually developed and implemented in the ambulatory care sector since the mid-1990s. An individual health insurance electronic card (Sesam-Vitale carte) is provided to all individuals enrolled in SHI. On the provider side, the billing system relies on an electronic identification card for health care workers (Carte de Professionnel de Santé). By 2012, 98% of doctors had such a card (Asip Santé, 2012).
DMPs were instituted by the 2004 Health Insurance Act (Loi No. 2004–810 du 13 août 2004 relative à l’assurance maladie), with the aim of grouping medical information gathered in ambulatory and hospital settings. After a long and costly phase of development and testing, the DMP was finally rolled out on a national basis in 2011. The decision to create a DMP is made by the patient on a voluntary basis, and participation has been very low: as of November 2013, only 5291 ambulatory health professionals and 378 health care facilities had incorporated the use of DMPs and 397 714 had been created.
Since January 2009, a system of patient pharmaceutical files (dossiers pharmaceutiques) has been progressively rolled out nationally. The file is created and accessed with the patient’s consent and allows pharmacists to check patients’ prescriptions within the previous four months, with the goal of preventing unnecessary prescriptions and contraindicated drug combinations. By December 2012, 98.4% of all pharmacies in France had installed the necessary equipment.
Certain hospitals, both public and private, offer the option of making appointments for consultations online. However, such systems are far from being generalized in France.
Because of the low professional interest in adopting electronic records, incentives have been put into place. The P4P provisions under ROSP (see section 3.7.2) include incentives for physicians to increase the use of information technologies in ambulatory care, including the electronic transmission of reimbursement claims by SHI and software for following patients and managing prescriptions.