30 January 2022 | Country Update
Changes in the funding reform of psychiatric care30 April 2021 | Country Update
Changes in funding for emergency departments11 May 2018 | Country Update
New measures to improve innovation in care models and funding13 March 2017 | Country Update
New financing modalities for critical care13 March 2017 | Country Update
New financing modalities to support the shift to ambulatory care28 September 2016 | Country Update
New medical contracts will cost more than a billion euros a year06 June 2016 | Country Update
Propositions for improving the DRG payment model23 March 2015 | Country Update
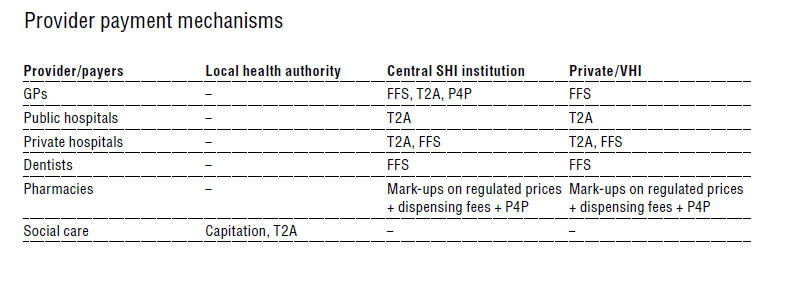
New payment scheme for multi-professional group practicesPayment mechanisms in the French health care system have long been based on FFS for health professionals working on a private basis and on prospective budgeting methods for health services. However, since the mid-2000s there has been a move towards the implementation of activity-based payment methods for health services, starting with the implementation of DRG tariffs in hospitals and the introduction of P4P for doctors, without impairing the FFS principle (Table3.9).
Table3.9
Interested health professionals, healthcare organizations (including from primary care), or legal entities, are invited to submit proposals to pioneer changes in the current funding and organizations rules of the health system. Article 51 of the 2018 Social Security Financing bill (decree n°2018-125, of 21 February 2018) gives the possibility of experimenting new funding and pricing models of healthcare, provided that pilots aim to improve quality and/or efficiency of care provision, care pathways or access to care. The selected proposals will need to take into account political priorities such as integrating health and social care pathways, improving the appropriateness and quality of care and enhancing access to care in medically underserved areas.
Selected vanguards will be conducted for five years, based on specifications currently being written. Further, a dedicated national Health System Innovation Fund of €20 million will be created. It will be supplemented by regional funds.
This measure is a first step for modifying the current activity-based payment model in hospitals in the context of increasing number of chronic conditions and fragmentation of healthcare organizations.
More information (in French):
https://www.legifrance.gouv.fr/eli/decret/2018/2/21/SSAS1736666D/jo/texte
A new decree (decree n°2017-247, of 30 February 2017) introduces new financing modalities for intensive and intermediate care units to better take into account the specificities of critical care. This care is characterized by considerable fixed costs due to operational requirements and by a fluctuating activity resulting from emergency situations. It was previously funded by supplementary daily packages on top of an activity-based payment (tarification à l’activité, T2A) through the French DRG system (groupes homogènes de séjours, GHS). The supplementary daily packages were provided for patients’ visits to intensive or intermediate care units which fulfilled several criteria (official approval of the unit, procedures undertaken during the visit and level of severity of the patient), and resulted in funding instability. Critical care will now be funded through a mixed model which will combine activity-based payment with an annual flat-rate fee based on the size of the units providing this care and their activity over the previous year. This annual fee will ensure a stable amount of resources covering the fixed costs of those units.
More information (in French):
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000034097103&dateTexte=&categorieLien=id
A new decree (decree n°2017-247, of 30 February 2017) introduces specific financing modalities for ambulatory care at the border between outpatient care and day care provided within hospitals. Such activities do not require a hospitalization but represent long visits which mobilize a number of staff from different fields. They include for example the global follow-up of diabetic patients which requires a visit from a diabetes specialist, a nurse, a dietician and an ophthalmologist. Previously, some hospitals charged the tariff of day care, which was far superior to the amount actually spent, or did not discharge hospitalized patients for those activities in order to compensate for the fact that certain costs (e.g. the intervention of paramedics) were not covered by the fee-for-service which funds outpatient care. To fill this gap, the new decree introduces an intermediate level of funding for those specific activities which will result in an estimated saving of €5 million and will support the shift to ambulatory care within hospitals by facilitating the development of those activities.
More information (in French):
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000034097103&dateTexte=&categorieLien=id
After months of tough negotiations, the Health Insurance Fund and the representatives of private doctors have recently signed a new agreement (25th August 2016). In total, nearly an extra 1 billion euros will be invested annually in ambulatory medicine by the public health insurance and an additional amount of 300 million euros by complementary insurances. This unprecedented effort decided by the Government, three months before presidential elections, aims above all to strengthen the general practice (primary care), access to and coordination of care.
Beyond the revaluation of tariffs or consultation fees (from 23 to 25 euros), different levels of consultations (30, 46 and 60 euros) have been defined to allow doctors to adjust the length of their consultation to patient’s need (children, chronically ill, older people). Extra payments are also planned to account for patient characteristics (age, pathology, etc.). To enhance access to timely care, the agreement financially encourages practitioners to accept a referred patient within 48 hours. Physicians will be further remunerated better on prevention, through increased payments on the current payment-for-performance scheme (ROSP).
More information (in French): http://social-sante.gouv.fr/IMG/pdf/16_25_08_-_cp_signature_convention_medicale_.pdf
MP (deputy) Olivier Veran, rapporteur of the Mission on the evolution of how health facilities are funded, presented a progress report to the Health Minister on 25 May. The report takes stock of the T2A, ten years after its implementation, and provides recommendations to change the initial model. Measures proposed include: a fixed guaranteed funding for small hospitals, completed by payments linked to activity; a partial activity-based payment for rehabilitation care facilities to “combine the dynamism and funding stability”; new “modulated payments” to support activities that fall outside the DRG logic and are currently inadequately addressed (for example, follow-up of chronic diseases, palliative care). The report also recommends: reconsidering the payments for emergency care, to encourage hospitals to transfer unscheduled visits to ambulatory emergency centres; revising the rules for day hospitalizations for medical cases; and simplifying the rules for coding. The report requests the 2017 health budget to consider these proposals to modify T2A. Additional recommendations on financing innovation and research and mental care will be issued in a final report in early 2017.
More information (in French): https://sante.gouv.fr/IMG/pdf/t2a_point_etape.pdf
Pursuant to the 2013 National Health Strategy, the Minister of Health introduced in February 2015 a new performance-based payment scheme for multi-professional primary care group practices (see Health Policy Update 26/03/2015). Practices voluntarily signing contracts with local SHI funds and regional health agencies will receive additional payments based on their results in terms of accessibility of health care, intensity of teamwork and utilization of computerized patient records. The contracts can provide up to approximately €52,000 annually (assuming a patient population of 4,000) in addition to the fee-for-service payments health professionals receive.
More information (in French): http://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000030289835&fastPos=4&fastReqId=1863389020&categorieLien=cid&oldAction=rechText
Generally, patients in the ambulatory care sector are expected to pay health care providers themselves and then claim reimbursement of a share of their expenses from their health insurance fund. However, there are situations in which the patient is exempt from making the initial direct payment. This system of direct payment by the health insurance fund to the provider is known as “third-party payment” (tiers payant) and is becoming increasingly common in ambulatory care. It currently applies to CMU beneficiaries and victims of occupational accidents, but under the planned 2015 Health Reform Law, it is expected to be extended to a larger part of the population. It may also be used in laboratories, pharmacies (for generic drugs only), hospital consultations and outpatient clinics, and by some doctors for expensive examinations and treatments.
All hospitals, except for long-term care and psychiatry, are funded using T2A, based on GHSs. Using data from the PMSI, each patient stay is classified in one of the approximately 2200 DRGs, and an associated GHS. Each GHS is subject to a lump-sum tariff that is set annually. GHS tariffs are calculated differently for public and private hospitals and do not include the same services (see below).
Within the T2A, there are two primary categories of hospital reimbursement: medical activity-based payment and non “activity”-based payment.
The medical activity-based category covers three areas:
Block grants and non “activity”-based financing cover three main areas:
In private profit-making hospitals, doctors’ procedures and services are not included in GHS tariffs and are paid separately, while they are included in the GHS tariffs for the public hospitals. Specific GHS tariffs are calculated for the private sector, together with an individual “transition coefficient” that aims to avoid large changes in hospital budgets from year to year and takes into account each hospital’s own historical costs/prices. Regional weights, similar to those of the public sector, are also used in the private sector, as well as a technical coefficient that applies to hospitals offering high-technology services.
Finally, special financing rules apply to hospitals in low-density, geographically remote areas that would otherwise be subject to consolidation because of low volume of use.
Psychiatric areas provide integrated inpatient and outpatient public mental health care, generally coordinated by a hospital specialized in mental health and paid on an annual prospective global budget basis, as are private psychiatric hospitals (see section 5.11). An information system, “summary of medical information for psychiatry” (recueil d’informations médicalisées en psychiatrie), has been implemented, but the payment mechanism (valorisation de l’activité en psychiatrie) is still being developed.
Outpatient care provided by self-employed GPs or psychiatrists is paid for on a FFS basis. Consultations for psychotherapy provided by other self-employed professionals are also paid on a FFS basis, but tariffs are freely set by providers because there is no coverage by SHI.
Outpatient pharmaceutical care is paid according to the official tariffs defined by CEPS (see section 2.8.4). Prices and payments for drugs are made on a package basis, and distribution of partial packages is prohibited even if it exceeds the number of units prescribed. However, under the 2014 Social Security Finance Act, a three-year voluntary project will test delivery of antibiotics on a unitary basis in retail pharmacies.
Drugs with marketing authorization that are not contained in the list of reimbursable drugs or for special drugs for inpatient care (see section 2.8.4) may be sold over the counter, with patients paying the full price, which is not regulated. Previously, VHI did not cover drugs not covered by SHI.
Inpatient pharmaceutical care is included in the GHS tariffs paid by SHI to the hospitals, with the exception of innovative expensive drugs, which are paid for on top of the GHS tariffs if listed on the special agreed products list.
On 1 January 2022, the reform for psychiatric hospital funding came into effect. The new funding model includes a capitation payment calculated for each region (based on the number of inhabitants, their socio-demographic characteristics, the number of psychiatrists, and the health and social care dedicated to psychiatric patients), an activity-based payment depending on the number of patients seen the previous year and the intensity of the care received, a bundle payment for specific activities, and additional payments to support research, quality of care, new activities, etc. The capitation payment is allocated to the regional health agency and then directed to psychiatric hospitals according to criteria that have yet to be defined in each region.
More information (in French), here: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000044126082
In 2021, the government announced that the payment model of emergency departments will be changed to consider the intensity and quality of emergency care in the payment and to improve the coordination of hospital and ambulatory emergency care. The new payment model consists of a capitation system (53% of the total budget) alongside activity-based payment (45%) and a small P4Q scheme (2%) that will be based on new emergency quality indicators to be calculated. Capitation is decided at the regional level based on the characteristics of the population, ambulatory care supply and other emergency departments within that region. Activity-based payment is based on a fee scale that varies with age, whether patients were brought by an ambulance, and their criticality, whether a specialist is consulted, and whether biological tests, radiology exams are necessary.
More information here (in French): https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043370640
Methods for paying health care professionals vary according to whether the professionals are self-employed in private practice or employed by institutions. However, some professionals such as doctors have mixed activities, and so their total remuneration may be a composite sum.
Self-employed professionals (GPs, specialists, dentists, nurses, physiotherapists, midwives, ambulance personnel, speech therapists, orthoptists and laboratory technicians) provide the vast majority of outpatient services and a large proportion of services in private hospitals and are paid directly on a FFS basis. Their gross income, therefore, reflects the number, type and price of the services they provide, minus their professional costs. Recently, new payment methods for particular tasks have been introduced. For example, a capitation system is used to pay for doctors’ management of patients with ALDs (€40 per patient per year), and currently there is experimentation regarding payment of health professionals involved in multidisciplinary provider networks.
Most health professionals are required to apply the statutory tariffs set out in the national agreements (conventions) (see section 3.3.4). However, there are exceptions, particularly for doctors with the permanent right to exceed the official tariffs (extra-billing). These are mainly doctors who have opted to work in Sector 2, as opposed to Sector 1 where the doctors are prohibited from extra-billing. In 2010, a quarter of doctors practised in Sector 2, although the proportion varies greatly among specialties (CNAMTS, 2011). Sector 2 doctors relinquish some of the social and fiscal advantages normally accorded by doctors under the agreements. Patients consulting a Sector 2 doctor are covered for the statutory tariff regardless of the level of extra-billing. Because extra-billing raises equity of access issues, access to Sector 2 is tightly controlled by SHI, and currently only doctors with certain full-time public hospital positions may request to access this sector. Because extra-billing can be very significant for certain specialties and in certain areas, impairing patients’ access to care, measures have been implemented to contain extra-billing (see section 6.1.2).
In 2009, SHI began to offer individual contracts on a voluntary basis to GPs that provided incentives for practice improvement. In 2011, this P4P scheme based on public health objectives (rémunération sur objectifs de santé publique; ROSP) was incorporated into the physicians’ collective bargaining agreement with an expanded list of objectives and extended to additional specialties. GPs participating in ROSP receive additional remuneration on top of their normal FFS income, which takes into account the size of the population treated by the doctor and 29 quality indicators with intermediate and final targets. Overall, the amount earned may exceed €7000 per year for a doctor achieving over 85% of the targets and treating more than 1200 patients. There is no penalty for the GPs who do not achieve the targets. In 2012, more than 89 000 physicians participated in the programme, receiving an average annual remuneration of €4215.
Doctors working in public hospitals are state employees who benefit from conditions of employment similar to civil servants. The method and amount of payment vary according to category.
University hospital doctors are authorized to devote a part of their working time to private practice within the hospital. Their fees are received by the hospital administration, which transfers them to the practitioner after withholding their own fees for use of facilities.
Since January 2000, pharmacists have been paid based on a mixed system linking a fixed-sum component (€0.53 per item) and a digressive sliding-scale margin; however, remuneration of pharmacists is evolving towards a fee-based system (honoraire de dispensation). Starting in January 2015, pharmacists will be paid a fixed sum of €0.80 per drug package (increasing to €1 in 2016), in exchange for a reduction in the price-based margins. Since 2013, pharmacists are paid for consultations with asthmatic patients and those treated with anticoagulants (€40/patient).
Pharmacists’ remuneration has also been used to support the development of the generic drug market. Since 1999, pharmacists have been authorized to substitute another drug from the same generic group for the one prescribed unless the doctor has noted “non-substitutable” on the prescription. The absolute mark-up paid for generics are the same as for brand-name drugs and higher manufacturer rebates for generics are allowed (maximum 50% of manufacturer’s list price versus 2.5% for brand name drugs). This policy has allowed for rapid expansion of the generic drug market, which in 2011 represented 24% of the reimbursable drug market in value and 13% in volume (IGAS, 2012a). In addition, a P4P scheme for pharmacists was initiated in 2013 with an initial focus on generics. Pharmacists are eligible for an annual bonus of up to €3000 depending on the share of generics delivered as well as the increase in this measure.