
31 August 2021 | Country Update
Extension of assisted reproductive technology10 January 2020 | Country Update
New reform to increase depth of coverage17 March 2016 | Country Update
Ensuring continuity of universal health coverage24 November 2015 | Country Update
Free care for victims of terrorist attacksThe 2016 Social Security Financing Act included a major reform to ensure life-long continuity of health coverage. The new Universal Health Protection (Protection Universelle Maladie; PUMa) is designed to ensure continuity of universal health coverage by reducing the administrative burden in proving eligibility for coverage and eliminating potential gaps in coverage due to changes in an individual’s professional, residential or family situation. Universal health coverage in France was achieved under the 1999 CMU Act, which covered all residents who previously had been ineligible. Effective 1 January 2016, PUMa extends this logic by simplifying the required proofs of eligibility. Employees now need only demonstrate that they are employed, regardless of duration. Non-employed individuals are covered if they reside in France on a stable and regular basis, and adults previously covered pursuant to a primary beneficiary’s eligibility will now have individual residency-based coverage. As a result of these simplified rules, the CMU basic coverage created for those not eligible on another basis will cease to exist. However, the CMU-C programme providing free complementary coverage will continue.
More information (in French):
http://social-sante.gouv.fr/affaires-sociales/securite-sociale/article/la-mise-en-place-de-la-protection-universelle-maladie-puma-au-1er-janvier-2016
Following the 13 November 2015 terrorist attacks in Paris, the Minister in charge of Health announced that the victims of terrorist attacks are immediately entitled to free care and simplified procedures to obtain daily indemnity allowances. These provisions were included in the draft 2016 Social Security Financing Act currently under consideration in the parliament and normally would become effective in 2016. The goal is to eliminate the administrative and financial burden on victims of terrorist attacks, who previously would have had to apply to the military SHI fund and would have received free care only if qualified for a disability pension. A special telephone number has been established so that the individuals affected may obtain more information about their personal situation.
More information (in French):
http://www.social-sante.gouv.fr
French SHI provides nearly universal coverage, with 99.9% of the population covered in 2013 (see section 2.3.5). Individuals are generally covered on an employment basis, and any dependants of the insured person are also covered. Employees cannot opt out.
For those not covered through one of the obligatory SHI schemes on an employment basis, the CMU Act offers SHI coverage to individuals who legitimately reside in France. CMU coverage is free for individuals with household revenues up to an established ceiling (€9534 in 2013–2014); other beneficiaries must pay an annual premium equal to 8% of revenues above the ceiling. Thus, coverage criteria have progressively moved from an employment basis to residency status. For transitory foreigners and undocumented migrants who have resided in France for at least three months, the AME provides free access to medical care for those with revenues below the CMU ceiling. Prisoners and their families are systematically covered by the SHI general scheme for the duration of the imprisonment.
Medical goods and services covered by SHI include:
In order to be eligible for coverage, diagnostic services, treatment, drugs and prostheses must be provided or prescribed by a doctor, a dentist or a midwife and dispensed by health care professionals or institutions recognized by SHI.
SHI provides benefits in-kind and in-cash. The benefit package in-kind covered by SHI is defined differently for outpatient and inpatient care. Covered outpatient goods and services are included in positive lists (Table3.5): the common classification of medical procedures for doctors (Classification commune des actes médicaux), the general nomenclature of medical procedures for other health care professionals (Nomenclature générale des actes professionnels), the list of reimbursable drugs (Liste des specialités pharmaceutiques remboursables) and the list of reimbursable medical devices and health materials (Liste de produits et prestations remboursables). There is no negative list.
Table3.5
For hospital inpatient care, there is a specific list for drugs (Liste des spécialités agréées aux collectivités), and the positive lists described above only apply for procedures reimbursed outside of the DRG system. In-hospital, expensive and innovative drugs and devices that are paid in addition to the DRG tariffs are included on special lists. For other categories of care, there is an implicit understanding of the range of services that can be delivered to patients because hospitals are paid on a DRG basis. Unless it is specified elsewhere (e.g. in a regulation or a specific guideline), hospital clinicians can decide what care to provide and what drugs to prescribe to patients (as long as drugs have AMM). Therefore, innovative procedures or products are often introduced first in hospitals (and not paid separately on top of the DRG system) and second inscribed on one of the lists mentioned above (lists included in Table3.5 or special lists for innovative care are paid for on top of DRG tariffs).
Initially, SHI focused on the coverage of curative care in case of illness or accident. In practice, however, preventive care is increasingly covered, particularly for services provided within doctors’ practices, such as mammography or cervical smear tests. Compulsory or recommended immunizations are also reimbursed, and care of pregnant women and newborn babies is free. A lump sum of €50 per year is available to smokers for smoking cessation products (€150 for pregnant women and young adults aged 20–25).
The range of services covered by SHI does not include cosmetic surgery or most thermal spa treatments (unless prescribed by a physician for one of the list of 12 specific conditions defined by SHI, such as rheumatic diseases, and subject to frequency and duration limits), nor does it include some services of uncertain effectiveness. The choices required in the allocation of scarce resources may result in non-reimbursement for certain procedures (e.g. bone densitometry performed in the private sector as a preventive measure) or limits on the frequency with which they can be reimbursed (e.g. mammography for screening purposes).
For most common health care or products, volumes of care are not specified. However, for expensive procedures or devices, volumes may be explicit. This is the case, for example, with respect to in vitro fertilization, for which four attempts are fully covered (the counter is reset in the case of a successful pregnancy) with an age limit of 42; or for drug eluting stents, with generally only one stent covered up to a maximum of three per patient in the case of acute occlusive artery dissection.
For certain kinds of care, such as physiotherapy and thermal spa treatments, prescription by a doctor is not a sufficient condition for reimbursement. Coverage for these kinds of treatment is subject to prior authorization by doctors advising the SHI Medical Service Office (médecins conseil du service médical), after examination of the patient’s case history and possibly a patient interview.
Cash benefits are also provided by SHI to compensate for sickness, maternity and paternity leaves, as well as in case of incapacity.
The positive lists are defined at the national level and apply throughout France in all regions. Drugs and medical devices are added to the list by the ministry in charge of health, while procedures are added by SHI (UNCAM) (see section 2.3.5) on the advice of designated committees of the HAS (see section 2.3.4) based on HTA results (see sections 2.7.2, 2.8.4 and 2.8.5). Key actors involved in defining the benefit package, the rate of coverage and pricing decisions are described in Table3.6.
Table3.6

While the French health care basket is considered very generous in terms of goods and services covered, coverage is generally not 100%. A share of the tariff is the patient’s responsibility and varies with the category of goods and services (see section 3.4). Moreover, SHI does not cover extra-billing amounts over the statutory tariffs (see section 3.7.2).
The SHI rate of coverage by type of care is as follows:
Inpatient care. The coverage rate for hospital care is generally 80%, but increases to 100% in a number of cases:
For treatments or tests with a tariff over €120, a flat-rate fee (participation forfaitaire) of €18 is applied instead of the generally applicable co-insurance amount, subject to the same exceptions listed above. This fee does not apply to diagnostic imaging, emergency transport or transport between care facilities (including HAD) and applies only once per hospital stay. Whatever the level of coverage of care, most patients must pay a flat-rate catering fee (forfait journalier) of €18 per day for hospital accommodation (€13.50 in mental health institutions), subject to the following exceptions: maternity care from the last four months of pregnancy until 12 days postpartum, newborns in the first 30 days, beneficiaries of CMU-C and AME, occupational injuries, HAD, disabled children under the age of 20 living in institutions, military pensioners, and those covered under the Alsace-Moselle SHI scheme. This fee may be covered by VHI.
Outpatient care provided by self-employed health professionals. Coverage rates range from 70% of the statutory tariff for health care provided by doctors and dentists to 60% for medical auxiliaries and laboratory tests. The €18 flat-rate fee for treatments with tariffs above €120 also applies to outpatient services in lieu of the applicable co-insurance amount. The flat-rate fee also applies if the cumulative cost of treatments provided within a single visit exceeds €120, but in any case cannot be applied more than once per visit. The reimbursement of services provided by medical auxiliaries and laboratory tests is conditional on a doctor’s prescription. However, in order to support the financial incentives to follow a coordinated care pathway, coverage of doctors’ visits can vary. Under the “preferred doctor” scheme, patients are requested to register with the doctor of their choice, whom they should see to obtain a referral to a specialist. The preferred doctor is most often a GP, but it may be a specialist of any kind working in the private or public sector. The coverage of patients who directly access specialists or other GPs outside of the coordinated care pathway falls to 30%.
Pharmaceuticals. Most drugs are covered at a rate of 65%, but this ranges from 100% for non-substitutable or expensive drugs to 15% for drugs judged to have a low SMR. Extra-billing for prescription drugs is not allowed and thus the market price is the same as the SHI statutory tariff.
Medical devices. Medical devices and prostheses are subject to various coverage rates depending on the medical device. The reimbursement rate is defined by reference to the statutory tariff, but manufacturers and distributors are free to set a price in excess of this tariff. In certain cases (e.g. spectacles, dentures, hearing aids), the reimbursement levels are particularly low.
As noted above, certain hospitalizations are covered for 100% of the statutory tariffs. Exemptions from co-insurance for all types of care apply in certain circumstances:
Exemptions on economic grounds do not exist. However, the free public complementary VHI coverage for people with low incomes (CMU-C; see section 3.5.1) effectively provides full coverage on an economic basis.
In order to raise additional revenue for SHI, flat-rate deductibles [2] were introduced in 2005: €1 (participation forfaitaire) is charged for every physician visit, laboratory test and diagnostic imaging up to an annual limit of €50. The list of goods and services to which deductibles (franchise médicale) apply was expanded in 2008 to include drugs (€0.5 per package), ancillary care (€0.5 per service up to a daily limit of €2) and medical transportation (€2 per transport up to a daily limit of €4). A second annual ceiling of €50 is set for these types of care. These deductibles do not apply to individuals under 18 years of age, beneficiaries of CMU-C and AME, and pregnant women from the sixth month. “Responsible” VHI contracts do not cover these deductibles (see section 3.5.3).
On 2 August 2021 a law was passed regarding bioethics (LOI n° 2021-1017 du 2 août 2021 relative à la bioéthique, 2021). In particular, it mandated the extension of assisted reproductive technology to all women, including single women and lesbian couples. In the first year of implementation of this law, the demand has been very high, resulting in long waiting times.
More information here (in French): https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043884384
In 2020, the reform “100% Health” (100% santé) was introduced to reduce OOP payments for dental care, optical and auditory equipment. A selection of basic dental care, dentures, eyeglasses and hearing aids are now fully reimbursed by the Statutory Health Insurance (SHI) and all Complementary Health Insurance (CHI), based on regulated prices.
This healthcare reform, also called the “zero excess” will be fully implemented by 2021.
More information (in French), here: https://solidarites-sante.gouv.fr/systeme-de-sante-et-medico-social/100pourcent-sante/article/100-sante-faciliter-l-acces-aux-soins-et-aux-equipements-auditifs-optiques-et
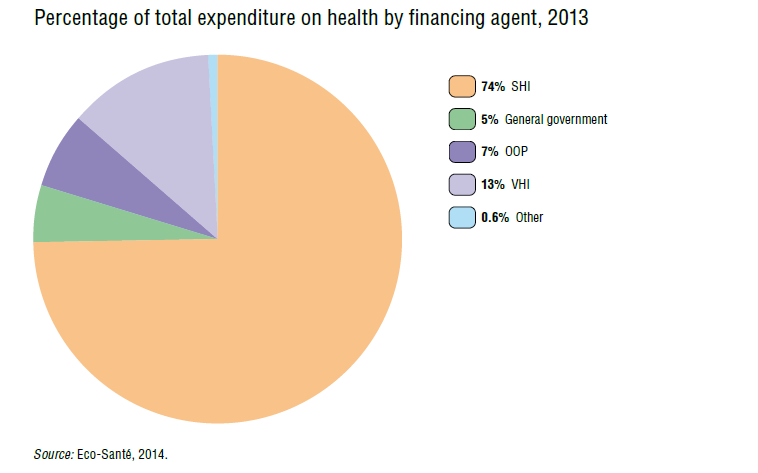
The state finances 4.9% of total expenditure on health (Fig3.6), and only 1.2% of expenditure related to personal health care consumption. The state finances activities in the areas of prevention (28% of state expenditure), medical research (30%), training of medical professionals (15%) and administrative costs of the health care system (7%). Other budget allocations are directed to the AME programme (see section 3.3.1), military hospitals, services for disabled veterans and emergency care (5%). Additionally, 14% of the state expenditure is directed to the CMU Fund for beneficiaries of CMU-C under the SHI funds (see section 3.5.4).
Fig3.6
Finally, the state also participates in SHI funding by subsidizing the exemption of employers’ SHI contributions in order to encourage employment of low-wage workers in domiciliary support services or in defined areas.
Between its inception in 1946 and 1998, SHI was almost exclusively funded by contributions from employees and employers as a proportion of wages and salaries, initially with a ceiling on contributions and later without a ceiling. The contribution rates for SHI have steadily increased to cover health care expenditure, which has grown faster than the level of overall contributions for social security. Between 1992 and 1997, contribution rates remained stable at 6.8% of gross earnings for employees and 12.8% for employers. In 2013, the employer contribution rate was 13.1%.
Since 1998, employees’ payroll contributions have been progressively replaced by an earmarked tax on all sources of income and have fallen from 6.8% to 0.75% of gross earnings in 2013. As a result of attempts to broaden the social security system’s financial base, employee’s contributions have been mainly substituted by the earmarked CSG introduced in 1991. The CSG rate varies depending on the source of income. Initially it was a two-tier rate but slowly evolved to a range, with higher rates for revenue from capital or from games of chance and a lower rate for revenue from those with low incomes. It is 7.5% on earned income (of which 5.29 percentage points goes to SHI), 8.2% on capital (5.95 percentage points for SHI), up to 12% on gambling winnings, 6.6% on pensions (4.35 percentage points for SHI) and 6.2% on benefits (e.g. unemployment and sick leave allowances) (3.95 percentage points for SHI). The rate decreases to 3.8% of earned income for individuals with low incomes who were otherwise exempt from income taxation, which represent nearly half of French households. Moreover, because the revenue base of SHI has been broadened and partly disconnected from earnings, it is less vulnerable to wage and employment fluctuations. A share of CSG contributions is generally deductible from income tax. In 2012, 70% of the revenues from the CSG went to the SHI schemes, accounting for 35% of their financing.
The pharmaceutical industry is also required to contribute through a 1.6% tax on their turnover, a tax on advertising, a tax on drug retailing and an additional tax if their turnover exceeds a limit set in the Social Security Finance Act. In 2012, these taxes raised €1.04 billion for SHI. Additional revenue for SHI is levied on the profits of companies with turnover of more than €760 000. This 0.13% tax is estimated to have levied €55 million in 2013. Other taxes are levied on polluting activities of companies. In 2012, employers’ contributions, employee’s contributions and CSG revenue accounted for 82.3% of total SHI revenue. The remainder was provided mainly through state subsidies and additional earmarked taxes (e.g. on tobacco and alcohol consumption).
The Union for the Recovery of Social Security Contributions and Family Allowances (Union de recouvrement des cotisations de sécurité sociale et d’allocations familiales) is in charge of collecting contributions and CSG at the local level. The money levied flows into a single national pool managed by the Central Social Security Agency (Agence centrale des organismes de sécurité sociale) and is distributed among the different national branches (SHI, retirement fund, family allowance, etc.) on the basis of contribution rates defined by law.
Since 1996, the contribution for solving social security debt, the social debt repayment contribution (contribution pour le remboursement de la dette sociale) was implemented to address the increasing deficit of the social security system. The contribution is 0.5% of revenue regardless of the source (earned income, benefits, capital, sale of assets, etc.). At the same time, a special fund was created to manage the social security debt, the Agency for Funding Social Security Debt (Caisse d’amortissement de la dette sociale). To ensure that the social security debt is not continuously transferred to the next generation, the parliament requires any new debt transferred to the Agency to be accompanied by an increase in the Agency’s income, ensuring that the time frame required to eliminate the debt is not extended.
Revenues for the CMU Fund, which finances CMU-C for low-income individuals as well as subsidies to purchase VHI for those with revenues up to 135% of the CMU-C ceiling (ACS) (see sections 3.5.1 and 3.5.4), mostly come from an earmarked premium tax on VHI contracts (€2 billion in 2012). The 2013 Social Security Finance Act added a fraction of the revenues from tobacco taxes (3.15%) to the CMU Fund.
SHI retrospectively reimburses care and, consequently, there is no formal resource allocation mechanism, although the creation of ONDAM (described below) acts as a soft tool to control and allocate health care expenditure. Because SHI schemes vary in their resources and population characteristics, health insurance schemes are subject to a financial adjustment mechanism that takes into account their demographic profiles.
Since 1996, the parliament has set a maximum national ceiling for SHI expenditure (ONDAM) for the following year, including spending limits for specific health care sectors (ONDAM subtargets), as part of the annual Social Security Finance Act.
In order to set the ONDAM for the coming year (n + 1), the government proposes an annual maximum growth rate for SHI expenditure. This rate is applied to the current year’s (n) actual expenditure. However, often the current year’s expenditure is a provisional estimate that is calculated in September, since voting on the ONDAM takes place before the end of the year. When genuine expenditure is known for year n, the change in expenditure in year n amounts to a ratification of overspending and to the integration of this overspending into the baseline used for defining the ceiling for the following year (n + 1).
Once the overall ceiling has been set, it is divided into five target groups:
Since the ONDAM target was introduced, priority has generally been given to the health and social care sector over the health care sector (see Table3.7).
Table3.7

From 1997 to 2003, there was significant spending in excess of the ONDAM. To address this problem, a parliamentary Alert Committee was created in 2004. If the system exceeds its projected budget by more than 1%, the Alert Committee may ask the Directorate of Social Security (the watchdog for all social security branches) to present a financial rescue plan. From 2003 to 2005, there was a lower degree of overspending achieved through better control of spending for ambulatory care and drugs. However, in 2006 overspending reached 1%, and in 2007 the alert procedure was used for the first time, resulting in the implementation of a range of cost-cutting measures in the fall of 2007. As a result, overspending was more moderate in 2008 and further reduced in 2009, despite the costs associated with two influenza epidemics: seasonal influenza in early 2009 and the H1N1 influenza A at the end of 2009. Since 2010, the ONDAM targets have been underspent (see Table3.7).
This target encompasses health professionals’ fees in private practice, including outpatient consultations in private hospitals, as well as prescription of drugs and medical devices, transport and per diem allowances for sickness and occupational accidents. SHI is responsible for ensuring compliance with the growth rates set by the government for these costs, which are included in the budget target agreed between the state and SHI.
During their annual negotiations with health professionals, SHI defines expenditure targets for each profession and measures to enable them to be met. To ensure that the professionals’ national agreements on statutory tariffs are consistent with the ONDAM target, the agreements are not implemented for a six-month period and the newly negotiated tariffs only become effective if the target is not exceeded. Otherwise, the previously negotiated tariffs remain in force.
The cost of medical goods prescribed in private practice is not directly regulated through the ONDAM. However, the annual Social Security Finance Act establishes a threshold rate of increase of the overall pharmaceutical companies’ turnover on reimbursable drugs: the K rate (taux K). Exceeding this rate results in financial penalties for pharmaceutical companies. However, there have been frequent criticisms of the discrepancy between the K rate and the ONDAM growth rate, the K rate being far below the ONDAM (0.4% for 2014 when the ONDAM was 2.4%).
This target encompasses spending by public and private hospitals paid on a DRG basis (T2A; see section 3.7.1) and other hospital spending. Since 2010, overspending the ONDAM hospital care target has been strictly prohibited. While the volume (case-mix) of hospital activity has far exceeded projections in recent years, the target has been underspent because of cancellation of reserve appropriations and lower than expected spending on other items within this target. Since 2013, a “prudential coefficient” has reduced the DRG tariffs for both public and private sector by 0.35%. This reserve may be partly or fully returned depending on the level of expenditure relative to the ONDAM target.
Although the ARSs have both a strategic planning and an oversight role with respect to hospitals (see section 2.5.3), their impact on hospital budget allocations is more limited. Of the €42 billion allocated by the ARSs in 2010, they had decision-making power with respect to only €2.9 billion (Cour des comptes, 2012c).
Budgets corresponding to the targets for health and social care for the elderly and disabled are transferred to the CNSA (see section 3.6). The budget for the elderly is used to finance health care costs and a share of social care cost in nursing homes (établissements d’hébergement pour personnes âgées dépendantes) as well as the community nursing services (Services de soins infirmiers à domicile; SSIAD). The budget for the disabled is used to finance nursing homes and SSIAD. Budgets are allocated to ARSs depending on service capacities in their geographical areas. The ARSs allocate budgets to services following the same principle (see section 2.5.1).
The ARSs are financed by a state appropriation (77%) and contributions from the SHI schemes (18%) and the CNSA (4%). The regional intervention funds were created under the 2012 Social Security Finance Act and combine these appropriations and credits to facilitate the capacity of ARSs to undertake transversal actions in the following areas: 24-hour services; experimentation and adaptation of care delivery, including multidisciplinary teams; working conditions in health care institutions; modernization and pooling of facilities, including information systems; and health promotion, educational activities and prevention, with a particular focus on loss of autonomy.
As already stated, SHI covers care provided by both public and private health care providers. Patients who consult these providers are reimbursed for a share of the cost of care (see section 3.3.1).
The relationship of independent health professionals with SHI is defined at the national level in agreements called “conventions” signed between UNCAM (SHI) (see section 2.3.5) and representatives of the professions. Conventions exist for doctors, nurses, physiotherapists, dentists, midwives, pharmacists, speech therapists, chiropodists, orthoptists, heads of biological laboratories, providers of transport and certain medical devices suppliers (e.g. opticians and orthodontists). In 2012, the first interprofessional agreement (accord cadre interprofessionel) was signed. It was designed to facilitate experimentation in coordinated care, with a particular focus on post-hospitalization patient care, care for patients with chronic or multiple diseases, and home care for dependent individuals.
All professionals are subject to the terms of the agreement unless they expressly opt out. In exchange, SHI pays a part of the professionals’ social security contributions. These agreements govern health professionals’ relations with patients who have public coverage and with SHI. The method of payment and the amount health professionals receive, therefore, should conform to the terms of these agreements or to the minimum contractual regulations that the government sets out in the absence of an accepted agreement. Agreements for each profession cover a period of four or five years or extend until a new agreement is signed. However, there are regular amendments (at least annual for doctors) that take into account changes following the yearly Social Security Finance Act and other new measures. The ministry in charge of health plays a significant role in the negotiation. Negotiations between SHI (UNCAM) and doctors tend to be very difficult because of the power of the medical professionals’ associations, with SHI rarely managing to implement the full range of measures it seeks.
In recent years, conventions have included several types of measure to promote quality and efficiency in the health system. P4P based on public health objectives was included in the 2011 collective bargaining agreement with physicians (see sections 2.8.3 and 3.7.2). Interestingly, the 2007 nurses’ agreement was used as a means of introducing controls on the geographical distribution of health professionals for the first time (other than pharmacists, for whom distribution has long been regulated). However, it was not followed by similar measures for other health professionals, in particular doctors (see section 6.1.3).
Purchasing relations with hospitals differ. The ministry in charge of health is responsible for public and private hospitals and sets the DRG tariffs. SHI reimburses hospitals on a case-payment basis in public hospitals, private non-profit-making hospitals and profit-making hospitals with a SHI agreement (cliniques conventionnées). For the very few private profit-making hospitals with no SHI agreement (cliniques non conventionnées), patients pay for their care directly and are reimbursed based on specific statutory tariffs called tariffs without consultation (tarif d’autorité), which are very low and have not been increased since the 1960s.