
Canada is a constitutional federation with sovereignty, authorities and responsibilities divided between the federal government and the provincial governments. With the exception of jurisdiction over hospitals and psychiatric institutions, which the constitution assigns exclusively to the provinces, the authority over health or medical care was never explicitly addressed in the original document, which, in the 1860s, assigned powers to the central and provincial governments. As a consequence, authority can only be inferred from a number of other provisions in the constitution. Subsequent judicial decisions support the view that the provinces have primary, but not exclusive, jurisdiction over health care (Braën, 2004; Leeson, 2004). As stated by Justice Estey in the Supreme Court of Canada case Schneider v. The Queen[6] “health is not a matter which is subject to specific constitutional assignment but instead is an amorphous topic which can be addressed by valid federal or provincial legislation, depending on the circumstances of each case on the nature or scope of the health problem in question”.
Although the three northern territories have a constitutional status that is subsidiary to the federal government, they have been delegated responsibility for administering public health care by the federal government. The federal government retains important “steering” responsibilities in terms of key dimensions of medicare through the Canada Health Act, the principles of which are upheld by provinces wanting to receive their full share of the Canada Health Transfer (see Fig2.1). By not taxing health benefits through employment-based insurance, the federal government also provides an implicit subsidy to encourage private health insurance coverage for non-medicare health services and pharmaceuticals. Fig2.1 is a highly simplified overview of the governance of publicly financed health care in Canada.
Fig2.1
Each province and territory has legislation governing the administration of a single-payer system for universal hospital and physician services (both in hospitals as well as those in ambulatory settings). Collectively, the 13 provincial and territorial health care insurance plans form Canada’s publicly funded health care system that has come to be known as medicare (Marchildon, 2009). In addition to paying for hospital care, either directly or through funding for health authorities (see Table2.3), provinces also set rates of remuneration for physicians that are negotiated with provincial medical associations (health authority budgets do not include physician services). Provincial governments also administer a variety of LTC subsidies and services as well as prescription drug plans that provide varying degrees of coverage to residents and mostly function as a safety net. These non-medicare services have grown over time relative to hospital and physician services.[7]
Table2.3

PT ministers of health are responsible for the legislation and regulations for the administration of universal coverage for medically necessary hospital and physician services. In some jurisdictions, there are two separate pieces of legislation, one pertaining to inpatient services and the other to medical services, while in other jurisdictions, both have been combined in a single piece of legislation. In provinces and territories with health authorities, some of the health minister’s authority and responsibility for the health system are delegated to public administrative agencies responsible for allocating resources for a broad range of health services (see Table2.3).
Regionalization combines devolution of funding from provincial ministries of health to the RHAs with a centralization of governance and administration from individual health care facilities and organizations to RHAs. In most provinces, RHAs act both as providers and purchasers of hospital care and LTC as well as other services delegated by provincial law. Between 2006 and 2018, Local Health Integration Networks (LHINs) in Ontario, unlike RHAs in the rest of Canada, did not provide services directly; instead, they allocated resources among hospitals and other independent health organizations. While in some cases RHAs facilitated horizontal integration, in particular the consolidation of hospitals, the main purpose of regionalization was to gain the benefits of vertical integration. By coordinating or integrating facilities and providers across a number of health sectors, RHAs were expected to improve the continuity of care and reduce costs by encouraging more upstream preventive care and, where appropriate, substituting potentially lower-cost home, community and institutional services for more expensive hospital care (Marchildon, 2016b). With funding from provincial ministries of health, RHAs and more centralized provincial and territorial health authorities (PTHAs) allocate health resources to serve the needs of their respective populations. However, no provincial government has delegated physician remuneration,[8] including family doctors who are responsible for the majority of primary care provision, or the administration of public prescription drug plans, to RHAs and PTHAs (Marchildon, 2016b).
The federal government plays a key role in setting pan-Canadian standards for UHC services – hospital, diagnostic, medical care, designated surgical-dental services and inpatient drug therapies – through the Canada Health Act (see section 3.3.3). The federal department of Health – Health Canada – is responsible for ensuring that the PT governments are adhering to the five criteria of the Canada Health Act. Although conditional transfers are a common policy tool in most federations, the use of the federal spending power in health care has been more controversial in Canada in large part because of the desire of some provincial governments and policy advocates for an even greater degree of fiscal and administrative decentralization (Boessenkool, 2010; 2013).
While PT governments must provide universally insured services to all registered First Nations and recognized Inuit residents, the federal government provides these citizens supplemental coverage for “non-insured health benefits” (NIHB) such as prescription drugs, dental care and vision care as well as medical transportation in order to obtain medicare services not provided on-reserve or in the community of residence. NIHB provide last-dollar coverage for those services not covered under an existing private health insurance programme (generally employment-based), PT extended benefit plans or other FPT social programmes.[9] Previously administered by Health Canada, the NIHB programme is now administered in a newly established department known as Indigenous Services Canada. However, Health Canada and the Public Health Agency of Canada (PHAC) continue to fund a number of population health and community health programmes in First Nation and Inuit communities (for example, the First Nations and Inuit Home and Community Care programme; and the Aboriginal Diabetes Initiative). Health Canada is also responsible for regulating the safety and efficacy of therapeutic products including medical devices, pharmaceuticals and natural health products and for ensuring food and consumer product safety. Data and patent protection for drug products is also administered by Health Canada under the Food and Drugs Act and the Patented Medicines (Notice of Compliance) Regulations under the Patent Act.
Since 2004, the PHAC has performed a broad array of public health functions including infectious disease prevention and control, surveillance, emergency preparedness, as well as leading national immunization initiatives, and coordinating or administrating programmes for health promotion, illness prevention and travel health. The PHAC is also responsible for regionally distributed centres and laboratories including the biosafety facilities at the National Microbiology Laboratory. The Public Health Agency of Canada Act also established the position of Chief Public Health Officer (CPHO). The Act empowers the CPHO to communicate with PT governments and their public health agencies as well as nongovernmental organizations (NGOs) and the private sector on public health issues. During the COVID-19 crisis in 2020, Canada’s CPHO Dr Theresa Tam worked with her PT counterparts to coordinate policy responses to the pandemic. During the pandemic, Dr Tam held daily live press conferences to give progress reports on the spread of COVID-19 and the responses recommended by her office to contain the contagion.
An arm’s-length quasi-judicial body – the Patented Medicine Prices Review Board (PMPRB) – regulates the factory gate price (defined as the price at which pharmaceutical manufacturers sell to hospitals, pharmacies and other wholesalers) of patented drugs. Established in 1987, the PMPRB acts as the consumer protection pillar of a major set of reforms to the Patent Act, which were designed to encourage greater investment in pharmaceutical research and development (R&D) in Canada through stronger patent protection. It is important to note that the PMPRB does not have jurisdiction over the prices charged by wholesalers or pharmacies, or over the professional fees of pharmacists. Although the PMPRB has no mandate to regulate generic drug prices, it does report annually to parliament on the price trends of all drugs (see section 2.8.4). In response to escalating prices of brand name drugs in Canada, and relatively high prices compared with other countries, in 2019 regulatory changes were made for the first time since the PMPRB was established (see Chapter 5).
In addition, the federal government plays a critical role in health research through the funding of the Canadian Institutes of Health Research (CIHR). CIHR is made up of 13 “virtual” institutes and provides research funding with the aim to improve health and strengthening the health system (Marchildon, 2013). While the majority of CIHR-sponsored research is investigator initiated, slightly more than 30% of CIHR-funded research is strategic, of which Can$ 115.9 million (€78 million)[10] was allocated to Government of Canada priorities in 2017–2018 (CIHR, 2018). The federal Minister of Health is responsible for CIHR and maintaining the objective of making Canada one of the five leading health research nations in the world. The federal government also provides the majority of funding for major research initiatives that are governed independently, including Genome Canada whose objective is to make Canada a world leader in research capable of isolating disease predisposition and developing better diagnostic tools and prevention strategies.
This research activity is supported by an extensive infrastructure for health data provided by Statistics Canada through five-year censuses as well as a number of health surveys. Recognized internationally, Statistics Canada was a pioneer in the gathering of health statistics as well as in the development of indicators of health status and the determinants of health. Data collection has been extended considerably through Statistics Canada’s partnership with the Canadian Institute for Health Information (see section 2.6).
As a decentralized state operating in an environment of increasing health policy interdependence, the FPT governments rely heavily on intergovernmental instruments to facilitate and coordinate policy and programme areas (Marchildon, 2010). Direct instruments include the (FPT) advisory councils and committees that report to the Conference of FPT Deputy Ministers of Health, which in turn report to the Conference of FPT Ministers of Health (O’Reilly, 2001). The federal government also provides funding for a number of specialized Pan-Canadian Health Organizations (PCHOs) which are summarized in Table2.4. In 2018, an external review panel (Forest & Martin, 2018) suggested major changes to the PCHOs including some potential mergers among the organizations, but at the date of writing, there have not been major changes to these PCHOs with the exception of the amalgamation of the Canadian Patient Safety Initiative and the Canadian Foundation for Healthcare Improvement in 2020 (Canadian Foundation for Healthcare Improvement, 2020a).
Table2.4
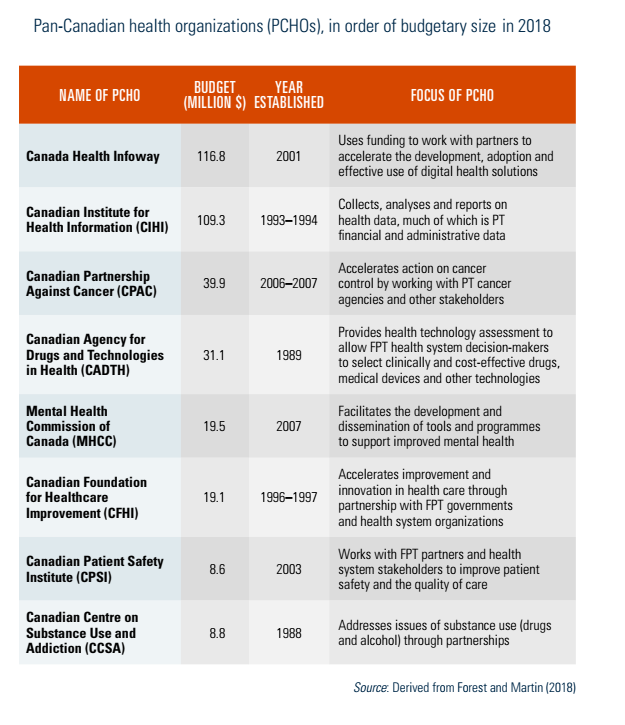
FPT governments collaborate extensively with civil society partners through the PCHOs (Table2.4). Working on projects with the Canadian Foundation for Healthcare Improvement, for example, PT governments regularly examine, implement and scale up innovations in health delivery in projects involving, for example, improving the health of LTC residents through more careful prescription of psychotics (Winnipeg Regional Health Authority), better self-management support for individuals with diabetes (Newfoundland), improving treatment for chronic care patients through telephone advice (Providence Health Care, Vancouver) (Canadian Foundation for Healthcare Improvement, 2020b). PT governments also work on projects involving mental health, cancer control and substance abuse on projects initiated or funded by the Mental Health Commission of Canada, the Canadian Partnership Against Cancer, and the Canadian Centre on Substance Use and Addiction.
Through the Council of the Federation, an intergovernmental organization established by the premiers of the 13 provinces and territories, PT governments created a Health Care Innovation Working Group made up of all PT ministers of health in 2012 (COF, 2016). In recent years, the Council has shifted its focus to cannabis legalization and regulation (COF, 2017).
Canadian health care programmes and policies are highly influenced by a number of NGOs. Many are organized as provincial associations and a number of these provincial bodies have national umbrella organizations that play an important role in facilitating and coordinating the memberships’ pan-Canadian initiatives. A significant number of national health NGOs also have charitable status, and they form some of the largest – as measured by revenues and tax-deductible donations – NGOs in the country, mainly hospital foundations and disease-based charities.
It is worth noting that, unlike countries with government-based health facility accreditation, Canada has a system of voluntary accreditation conducted by an NGO (Shaw et al., 2013). Known as Accreditation Canada, this NGO accredits hospitals, health facilities and health authorities as well as conducts reviews and assessments of health facilities and regional health systems with recommendations for improvements.
Health provider organizations have played a major role in shaping health care policy in Canada. For example, the Canadian Medical Association (CMA) is the umbrella national organization for physicians, specialists and general practitioners (GPs) – known as family doctors in Canada. In addition to lobbying for its members’ interests, the CMA also conducts an active policy research agenda and publishes the biweekly CMAJ (Canadian Medical Association Journal) as well as six more specialized medical journals. The 12 PT medical associations (Nunavut is not represented) are self-governing divisions within the CMA. These PT bodies are responsible for negotiating physician remuneration and working conditions with PT ministries of health, except in Quebec where negotiations are carried out by two bodies representing specialists and GPs. While the CMA is not involved directly in such bargaining, it does – when called upon – provide advice and expertise to the PT associations.
The role of the CMA and, in particular, its provincial divisions, must be separated from the regulatory role of the provincial colleges of physicians and surgeons including licensing, setting standards of practice, investigation of patient complaints as well as enforcement. As is the case with most professions in Canada, physicians are responsible for regulating themselves within the framework of provincial legislation. A national body, the Royal College of Physicians and Surgeons of Canada (RCPSC), restricts its function to overseeing and regulating postgraduate medical education.
The Canadian Nurses Association (CNA) is a federation of 11 PT registered nurses’ organizations with approximately 139 000 members as of 2018.[11] Some of the provincial organizations, such as the Registered Nurses Association of Ontario, have considerable policy and regulatory influence within their respective jurisdictions. Since nurses are highly unionized in Canada, their provincial and territorial union organizations exert considerable political influence. The unions are represented at the national level by the Canadian Federation of Nurses Unions.
There are numerous civil society groups at the pan-Canadian level the chief objective of which is to mobilize support and funding for both general and specific health care causes. Other charitable organizations promote a greater public focus on particular diseases or health conditions through advocacy, information and advice for affected individuals and their caregivers. Many of these organizations have charitable status and provide funding for research in their respective areas.
Finally, there are industry associations that represent for-profit interests in health care. These include organizations such as the Canadian Generic Pharmaceuticals Association, Innovative Medicines Canada (the organization representing the patented, research-based pharmaceutical companies), and the Canadian Life and Health Insurance Association.