-
01 January 2020 | Country Update
Introduction of DRG system in psychiatric hospitals -
23 October 2019 | Policy Analysis
Federal Council adopts cost containment measures -
30 September 2018 | Policy Analysis
Outpatient care takes precedence over inpatient care – six groups of surgical interventions to be moved to outpatient care -
13 November 2017 | Policy Analysis
Revision of the reimbursement scheme of ambulatory care (TARMED)
3.7. Payment mechanisms
In January 2018, the Federal Council implemented TARPSY, a lump-sum-based tariff system regulating the payment of inpatient psychiatry services. This system intricately associates treatments and services with specific cost-groups (PCGs) based on medical and economic criteria, remunerating through daily lump sums. Uniformly applied throughout Switzerland, TARPSY covers all aspects of inpatient psychiatric care for adults, with mandatory application in child and adolescent psychiatry since 2019.
Continuously refined since its inception, TARPSY releases an annual updated version, incorporating precise grouping logic, recent data, and adaptations to clinical practices and hospital settings. The PCG Catalogue complements this system by providing comprehensive information on evaluations related to cost-groups, ensuring compliance with TARPSY billing rules and definitions. Supplementary fee indications allow for the billing of additional fees in accordance with specified guidelines.
Crucially, the PCG Catalogue discloses the cost-weight for each day, determined by multiplying the length of stay by daily cost-weights, offering transparency in understanding the financial aspects of inpatient psychiatric care.
Authors
References
Federal Office of Public Health FOPH. Il Consiglio federale approva le strutture tariffali nazionali. Retrieved from: Federal Office of Public Health FOPH: https://www.bag.admin.ch/bag/it/home/das-bag/aktuell/medienmitteilungen.msg-id-86214.html
SwissDRG SA. Catalogo PCG. Retrieved from: swissdrg.org: https://www.swissdrg.org/de
Context & Impetus
To contain constantly growing health costs, the Swiss Federal Council adopted a cost containment program based on an international expert report in March 2018. The Federal Department of Home Affairs was commissioned to assess and implement new cost containment measures.
Reform Measures
A first of two sets of measures was adopted by the Federal Council in August 2019. The nine measures address all sectors and actors in the health system and are expected to result in substantial cost savings.
Experimental article
An experimental article will allow cantons and collective bargaining partners to implement innovative but timely limited cost-cutting pilot projects outside the Federal Act on Health Insurance (KVG).
National tariff organisation
Tariff partners are legally required to set up a national tariff organisation responsible for tariff structures in ambulatory care. This aims to strengthen day-to-day partnership and to resolve existing blockades in the ambulatory sector, for example, with the tariff structure TARMED. Service providers are obliged to provide data free of charge.
Keep tariff structure up to date
The tariff partners and the new tariff organisation are legally required to provide the Federal Council or the cantonal government data required to specify, adapt, and approve tariff structure and prices.
Promoting capitation payments in ambulatory sector
Capitation payment tariffs in the ambulatory sector are to be based on a single and uniform tariff structure agreed throughout Switzerland, similar to fee-for-service tariffs.
Measures to control costs
Service providers, insurers, and their associations are legally required to agree on cost-control measures in contracts valid throughout Switzerland.
Reference price system for medicinal products
Generic medicine in Switzerland is twice as expensive as in comparable European countries. A reference pricing system for patent expired medicinal products will be introduced. If at least three medicinal products with the same composition of active substances are on the positive list, a reference price will be defined for the active substance concerned.
Invoice copy for insured persons
Service providers will be legally required to provide insured persons a copy of the invoice, allowing patients to regain consciousness of costs of medical care. The service provider can be sanctioned if he fails to comply.
Maximum amount of penalties
The compulsory health insurance (KVG, Art. 59(1)) contains penalties applicable to service providers that violate legal requirements or contractual arrangements in respect to cost-effectiveness and service quality, as well as rules on invoicing. The maximum penalty may amount CHF 20 000.
Insurers’ right of appeal regarding hospital planning decisions
Insurers’ organisations are to be granted right of appeal against decisions of cantonal governments regarding planning and lists of hospitals, birth homes, and nursing homes. Previously, only service providers affected by the planning had the right to appeal.
Authors
References
Federal Office of Public Health (2019). Bundesrat beschliesst neun Massnahmen gegen höhere Kosten im Gesundheitswesen. [Federal Council adopts nine measures against higher health care costs] https://www.bag.admin.ch/bag/de/home/das-bag/aktuell/medienmitteilungen.msg-id-76105.html, last accessed: 24 September 2019
Federal Office of Public Health (2019). Massnahmen zur Kostendämpfung – Paket 1: Übersicht. [Measures to reduce costs – Package 1: Overview] https://www.newsd.admin.ch/newsd/message/attachments/58122.pdf, last accessed: 10 October 2019
Context
Compared to other countries, Switzerland has a high level of inpatient activity and has experienced considerable difficulties moving surgical procedures to an outpatient setting, even in cases where outpatient procedures are medically appropriate and require fewer resources. OECD data from 2008 show that the proportion of surgical procedures undertaken in the hospital outpatient setting was slightly less than 20% compared to more than 60% in the US or between 50% and 60% in the UK, Netherlands and Denmark.
Even though outpatient procedures are becoming increasingly common in Switzerland, the proportion of outpatient surgeries in relation to all surgical procedures performed in hospitals remains low.
Impetus
The Swiss Federal Office of Public Health (FOPH) commissioned the Swiss Health Observatory (OBSAN) to estimate the potential for shifting procedures to an outpatient setting and the associated cost implications. Based on criteria set out by the FOPH, namely (1) that the length of any inpatient stay following an outpatient procedure can last no more than two nights, and (2) these outpatient procedures are only considered for patients without complications or comorbidities, the OBSAN estimated that 33,000 inpatient cases in 2016 could have been carried out in an outpatient setting. Considerable savings could be expected for cantons because they contribute 55% of the costs of treatment, while outpatient services are financed entirely by the insurers. In fact, savings were estimated by the OBSAN to amount to more than 90 million Swiss francs (77 million euros).
Reform
In February 2018, the Federal Department of Home Affairs decided that the following six groups of interventions would only be reimbursed if undertaken on an outpatient basis:
- Unilateral varicose vein surgery of the legs
- Hemorrhoid procedures
- Unilateral inguinal hernia surgery
- Examinations/interventions on the cervix or uterus
- Knee arthroscopy, incl. arthroscopic surgery on the meniscus
- Tonsil and adenoid surgery
The aim of the decision is to create uniform regulations for all insured individuals in Switzerland who undergo these procedures. The corresponding amendment to the “Health Care Benefits Ordinance” (Krankenpflege - Leistungsverordnung – KLV/OPAS) will come into force on 1 January 2019.
Hospitals and insurers must adapt to the new regulations by January 2019. Criteria are being developed to determine exceptional cases in which inpatient treatment can continue to be reimbursed.
Furthermore, a plan is being developed to monitor changes in the number of inpatient and outpatient interventions in order to assess the impact of the reform. This is part of a larger evaluation to be undertaken over the next three years which will assess the effects of the reform on patients, service providers and insurers with regard to quality and costs. Subsequently, a decision will be taken whether to expand the list of outpatient surgical interventions. In the meantime, some cantons (in particular Aargau, Lucerne, Valais, Zug and Zurich) have already introduced their own lists, which include more interventions than the six set out above.
Authors
References
Federal Office of Home Affairs. 07.06.2018. Verordnung des EDI über Leistungen in der obligatorischen Krankenpflegeversicherung (Krankenpflege-Leistungsverordnung, KLV). https://www.admin.ch/opc/de/official-compilation/2018/2361.pdf, last accessed 20.07.2018
Federal Office of Public Health. 20.06.2018. Änderung der Krankenpflege-Leistungsverordnung (KLV) betreffend "Ambulant vor Stationär". https://www.bag.admin.ch
Schwendener, P., & Sommer, P. (2016). Ambulant vor stationär. Oder wie sich eine Milliarde Franken jährlich einsparen lassen. https://www.pwc.ch/de/publications/2016/ambulant_vor_stationaer_de_16_web_final.pdf, last accessed 20.07.2018
OECD Health Statistics. http://www.oecd.org/els/health-systems/health-data.htm, last accessed 20.07.2018
Swiss Health Observatory. 20.02.2018. Verlagerungspotenzial von stationär zu ambulant. Analyse ausgewählter chirurgischer Eingriffe. Studie im Auftrag des Bundesamtes für Gesundheit (BAG). https://www.obsan.admin.ch/de/publikationen/le-potentiel-de-transfert-du-stationnaire-vers-lambulatoire, last accessed 20.07.2018
Context
Since 2004, ambulatory care covered by mandatory health insurance is uniformly reimbursed based on a fee-for-service scheme called TARMED (tarif médical). TARMED is a joint project of all health care providers and health care financers, i.e., the association of medical doctors (FMH), health insurers (santésuisse and curafutura), hospitals (H+) and the national social insurances (accident, disability and military insurance). Since its introduction, only single positions of TARMED have been adjusted but no general revision of the tariff structure has ever taken place. The need for a comprehensive revision of TARMED is undisputed but the tariff partners so far have not found an agreement on a new reimbursement scheme.
Impetus
Given that no revision had taken place until 2017, the Swiss Federal Council intervened and implemented an adjusted TARMED, which will enter into force at the beginning of 2018.
Reform
With the revision of the reimbursement scheme, the Federal Council estimates to save yearly 470 Mio. CHF. The reform stipulates 10 measures that revise the reimbursement rates and simplify tariff positions. This includes, among others, the following modifications:
- Harmonization of tariffs across medical specializations. Until
now, the tariff varies across medical specializations as they aimed to
account for the differences in the duration of education for medical
specializations. Due to a harmonization of the education of medical
specializations, these tariff differences are no longer legitimate.
Thus, the reform will harmonize the reimbursement rates across
specializations.
- Reduced rates for technical services. Over
the past years, advancements of medical technology have increased
productivity in the field of surgery. To account for this, the reform
will decrease reimbursement rates for procedures with medical
technology.
- Reduction of maximum reimbursed consultation time. For certain treatments, the maximum reimbursed consultation time will be reduced to increase productivity of care providers.
- Reduction of services in absence of the patient.
To increase transparency, medical doctors will now be obliged to
indicate exact tariff positions for services when the patient is not
present. In addition, the maximum time the medical doctor is allowed to
charge for services when the patient is not present will be reduced.
Authors
References
Federal Office of Public Health. 18.10.2017. Factsheet – Anpassung des Ärztetarifs TARMED. https://www.bag.admin.ch
3.7.1. Paying for health services
The main provider groups and corresponding payment methods are shown in Table3.8. FFS is the dominant method of provider payment in Switzerland. For inpatient care, DRGs have replaced per diems as the most important payment mechanism; for long-term care a system of care-level adjusted per diem payments exists. Public health activities are mostly paid for on the basis of lump sum contracts or FFS.
Table3.8
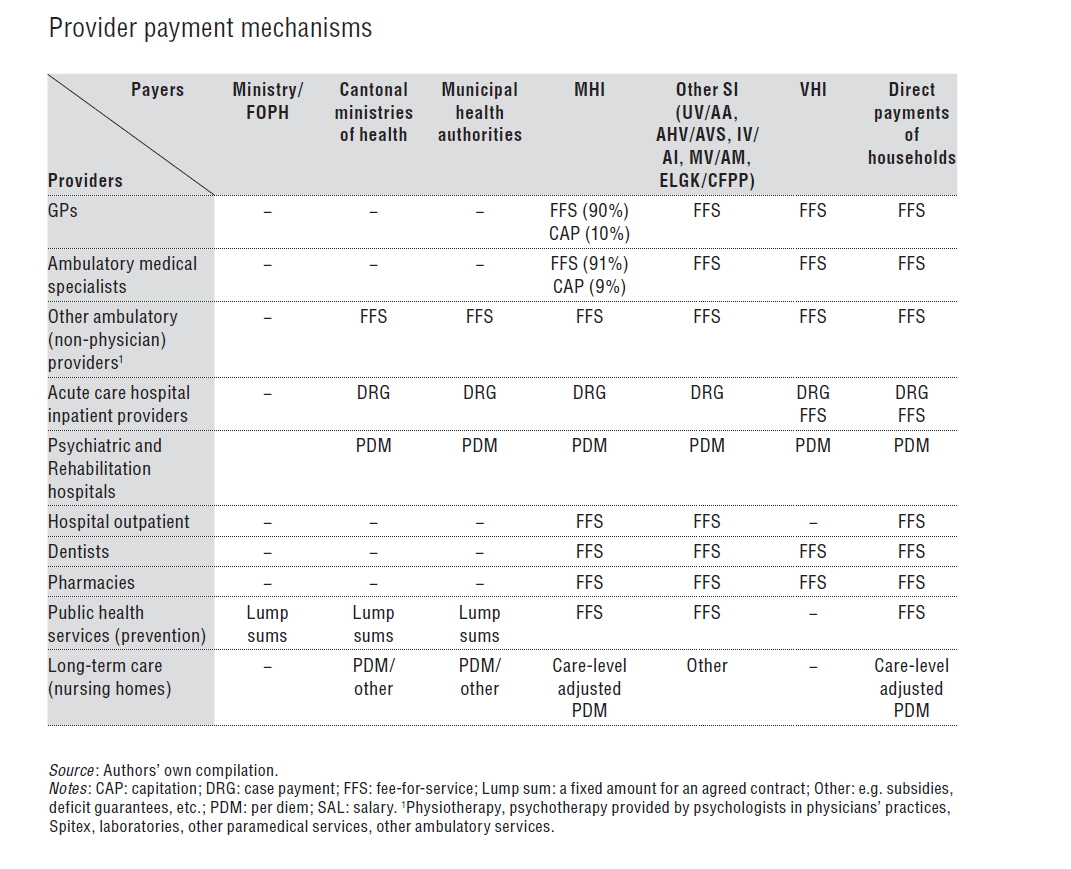
Ambulatory care
FFS is the dominant payment mechanism in the ambulatory sector. Volume limits on the number of billable services do not exist.
All medical doctors (GPs and specialists) with a practice authorization are reimbursed for MHI-covered services (and also for services reimbursed by other SI or households) on the basis of the nationally uniform FFS system TARMED (derived from tarif médical). TARMED is a relative value scale, and weights for each service item (locally referred to as “tax points”) consist of two parts: (1) the medical part for physicians; and (2) the technical part for technical and nursing staff, equipment and overheads. The medical part was calculated based on estimates of experts (representatives of specialist associations) about the necessary physician time for providing the services and an annual reference income of Sw.fr.207 000 (with adjustments for specialty and additional qualifications). TARMED tax points are converted into monetary values by multiplication with the negotiated cantonal point value. This value varied in 2014 between Sw.fr.0.82 in the cantons of Lucerne, Schwyz, Valais and Zug, and Sw.fr.0.97 in Jura. For more information about negotiations about point values, see section 3.3.4.
TARMED was introduced in 2004 as the basis of reimbursement for MHI-covered services after it had already been used by other social insurers since mid-2003. The aim of TARMED was to harmonize reimbursement of providers working in different cantons and different settings in order to remove some of the perverse incentives, which distorted the choice of care setting, i.e. shifting ambulatory patients between hospital outpatient departments and physicians’ practices. In addition, the introduction of TARMED aimed to improve reimbursement for GP services by giving greater weight to non-technical services than to technical services, and incentivizing less resource-intensive forms of care. Nevertheless, the problem of comparatively low reimbursement for GPs has remained on the political agenda. TARMED is regularly updated by the corporatist institution TARMED Suisse (see section 2.3.6). However, in June 2014, when payers and providers represented within TARMED failed to agree on a revision of the fee schedule, the Federal Council mandated a change to TARMED, resulting in increased reimbursement for primary care physicians (FOPH, 2014l). This was the first intervention of the Confederation on the basis of a new subsidiary competence (Art. 43, 5bis KVG/LAMal) received as a result of a reform in January 2013 (see section 7.5.1).
Although FFS is the dominant payment mechanism, capitation payments are gaining increasing importance. In 2012, about 10% of the MHI costs of GPs and 9% of specialists were reimbursed in the form of “capitation-type” payments (SASIS, 2014). These were made to HMOs or networks of physicians providing services in the context of managed care type insurance contracts. Under these contracts, a global budget based on risk-adjusted capitations (with adjustments for age, sex and other characteristics of the insured population) is usually agreed between an MHI company and providers carry at least partial budget responsibility for their subscribed patients.
Hospital outpatient acute care is also paid FFS on the basis of TARMED points and the negotiated cantonal point values. Point values are different for physicians in ambulatory practice.
Other MHI-covered ambulatory services provided by non-medics, such as physiotherapists, (psychological) psychotherapists working in physicians’ practices, laboratory and other paramedical personnel, are also paid for on a FFS basis. All professions in the ambulatory care sector have a nationally agreed fee schedule, which is negotiated between the relevant professional association and the association of MHI companies (or other social insurers such as UV/AA, MV/AM, AHV/AVS and IV/AI).
Home care (Spitex) services are reimbursed by MHI with Sw.fr.54.60 per hour for basic care services; Sw.fr.65.40 per hour for assessment and treatment; and Sw.fr.79.80 per hour for health checks, counselling and coordination. The maximum MHI contribution per patient is Sw.fr.79.80 per day, and patients have to cover up to Sw.fr.15.95 per day, with any remaining costs covered by the cantons or municipalities.
Services not covered by MHI are financed by VHI or by direct payments of patients on a FFS basis. Actors are – in principle – free to negotiate fees for services. For example, providers can add a certain percentage increase to the normal TARMED fee schedule. For services that are not specified by TARMED (e.g. alternative medicine), fee levels are determined freely by providers.
Dentists providing outpatient dental care services in Switzerland are financed almost 90% from OOP payments from patients, with the rest coming from private insurances (VHI) and from SI (MHI, UV/AA, IV/AI, MV/AM). If paid by SI, the invoices are calculated based on a national dental FFS system (called dentist tariff SSO), which is also a relative value scale specifying a certain weight (points) for 500 service items. The point value paid by social insurers is the same for all dentists in Switzerland, i.e. Sw.fr.3.10 in 2015. If patients or VHI cover the costs, dentists can increase (or decrease) the point value up to Sw.fr.5.80 (and there is no bottom limit).
Hospital inpatient care
Since January 2012, acute care hospitals are paid on the basis of the national SwissDRG system. Cantons bear between 51% and 55% of the costs of each inpatient admission in 2015, and their share will increase to at least 55% in all cantons by 2017. MHI companies pay for the rest. Actual hospital payment still varies considerably across cantons and may also vary across hospitals within cantons (e.g. university versus other hospitals), depending on the individual hospital base rates (for an overview of base rates, see GDK/CDS, 2015b). If patients choose to be treated in a hospital in another canton with a base rate that is higher than the base rate that would have been paid in the canton of residence for the same service (the reference rate), the difference may have to be covered by patients out of pocket or by VHI (see section 5.4).
DRG-based hospital payment was introduced in Switzerland as a result of a revision of the KVG/LAMal adopted by Parliament in 2007 (see section 6.1.2). The aim was to harmonize hospital payment across cantons (as well as for public and private hospitals) and to improve transparency and efficiency. Previously, large differences had existed in hospital payments for similar services across cantons, with hospitals in some cantons being paid on the basis of per diems and in others on the basis of DRGs, and with public (or subsidized hospitals) receiving direct cantonal funding for investments and education (and possibly deficits). Harmonizing hospital payments across cantons was an important step towards improving choice of hospital for patients seeking care in a canton other than their canton of residence.
The SwissDRG system has been developed by SwissDRG SA (see section 2.3.6) on the basis of the German DRG (G-DRG) system and data collected from an increasingly large sample of Swiss hospitals: 39 hospitals contributed data in 2007 (accounting for about 60% of hospital activity) and this number increased to 112 hospitals in 2014. The G-DRG system was adjusted to the Swiss context (amongst others to the Swiss Procedure Classification System, CHOP). National DRG weights, which are indicators of the relative costs of treating patients in one DRG when compared to the average costs of treatment of all patients, are calculated based on Swiss cost data. Investment costs are included in DRG-based payments since 2012 (by adjusting the base rate), and DRG weights include investment costs since 2015 (see section 4.1.1). Costs for research, university-level education and the costs of ensuring geographic availability of hospital capacity are excluded (Fischer, 2014).
Mental health (psychiatric) and rehabilitation hospitals are not yet paid on the basis of casemix systems (similar to DRGs). They continue to operate under a per-diem system. Originally, it was intended that psychiatric and rehabilitation hospitals would also transfer to a casemix-based payment system by January 2012 (as prescribed by the law). However, because these systems had to be developed from scratch (as international systems were unavailable), the new payment systems are still in the pilot stages (Caminada et al., 2015). It is currently envisaged that both psychiatry and rehabilitation will transfer to a new payment system in 2018 for the entire country.
Pharmacies (outside hospitals)
In 2001, the remuneration of pharmacies was changed from a simple proportional mark-up scheme to a mixed payment system consisting of a regressive mark-up included in the retail price of pharmaceuticals, which is specified in the positive list (see section 2.8.4), and a small number of fees for certain services. Most importantly, there is a basic fee of Sw.fr.3.25 (in 2015) per patient contact and a fee per dispensed prescription of Sw.fr.4.30. In addition, fees exist for specialized services, e.g. for a polymedication check (for patients taking more than four medications at the same time); for monitored medication intake; for methadone replacement therapy; and for substituting an original brand drug with a cheaper generic. The latter is reimbursed with an amount that depends on the price difference between the branded drug and the generic (capped at a maximum of Sw.fr.21.50).
The aim of this new reimbursement was to improve cost-effectiveness in the use of medicines and to overcome unintended consequences of a link between the payment of pharmacists and the financial volume of dispensed medicines (Vaucher & Rohrer, 2015). In 2010, the system was slightly updated.
Public health services
Public health services (prevention measures against alcohol, tobacco and drug abuse, infectious disease control and accident prevention, as well as food quality control and school health programmes, etc.) are often contracted out by cantons or municipalities to non-profit organizations, which receive a lump sum for a set of prevention measures specified in a contract. Payment of MHI companies (e.g. for vaccinations) and direct payments by private households are mainly FFS. Donations and bequests to non-profit organizations may be linked with specific requests of the funding organization.
Institutional long-term care
Since January 2011 (see section 6.1.4), medically indicated care provided at nursing homes is paid by MHI in the form of a flat rate of Sw.fr.9.00 per day and per care level, which is determined by the degree of dependency (see section 5.8). The maximum daily MHI contribution (for care level 12) is Sw.fr.108 and is fixed by the federal government (Federal Council). If the amount reimbursed by MHI does not cover the total medical costs, patients pay up to 20% of the maximum MHI contribution, i.e. a maximum patient contribution of Sw.fr.21.60 per day or Sw.fr.7884 per year, for institutional long-term care. These patient payments are usually made in the form of flat rates per day, depending on the degree of dependency. Any remaining costs are financed by the canton or municipality (see section 5.8.2 for the distribution of costs across payers).
For nursing homes that are publicly co-financed or subsidized, the public (cantonal or municipal) contribution is usually linked with a contract that specifies certain requirements (e.g. the provision of high-quality care). However, the details of these contracts can be manifold (deficit guarantees, infrastructure investments, etc.) and requirements are often relatively unspecific. Patient contributions for assistance and housing are usually lower in publicly co-financed or subsidized institutions compared with private institutions.
3.7.2. Paying health workers
Physicians
The income of doctors in independent practice is directly determined by the payment system as described in section 3.7.1. In some cantons, these doctors are allowed to run a practice pharmacy, which can generate an important share of the total income (see section 5.6.2). The annual median income of physicians in independent practice was around Sw.fr.190 500 in 2009, with considerable variation across regions (Sw.fr.181 100 in Zurich and Sw.fr.244 050 in Central Switzerland) and specialties (Sw.fr.107 400 for child and adolescent psychiatrists and Sw.fr.374 400 for gastroenterologists) (Kraft & Laffranchi, 2012). For comparison, the annual median income across all sectors of the economy was Sw.fr.77 268 in 2012 (FSO, 2015b).
In insurance-owned HMOs (see section 5.3), doctors are employed and receive a salary. In doctor-owned HMOs, doctors normally receive performance-related payments as well as a guaranteed minimum income.
Most physicians working in hospitals are employed and receive a salary, independently of whether they work in inpatient or outpatient departments. The average annual salary of assistant doctors (in specialization training) was estimated to be around Sw.fr.101 000 in 2010, while that of specialist doctors was Sw.fr.163 000 (Künzi, Strub & Stocker, 2011). Salaries of managing doctors were at Sw.fr.293 000 and chief physicians earned Sw.fr.419 000, with considerable parts of their salaries (about 42% of the salary of chief physicians) determined by bonuses. Bonuses are generated mostly through the provision of services to inpatients with VHI, and they are increasingly redistributed by hospitals across employed physicians.
Other professionals in ambulatory settings
Most professionals in an ambulatory setting – pharmacists, chiropractors, physiotherapists, ergotherapists, dentists, nurses, midwives, speech therapists and nutrition advisers – are either in independent practice or members of the staff in independent practices. Therefore, their income is directly determined by the payment system as described in section 3.7.1.
Nurses and midwives in hospitals or nursing homes
Nurses, midwives and assistant nurses working in hospitals and nursing homes are almost always employed and receive a salary. There is relatively little information available on salary levels of nurses. According to pflege-berufe.ch, the average salary of nurses in the Canton of Zurich was between Sw.fr.62 600 and Sw.fr.74 400, depending on the type of education (University of Applied Sciences or College of Professional Education and Training).