-
31 July 2025 | Country Update
Adoption of the National Strategy for Health Literacy -
20 February 2025 | Country Update
New “right to be forgotten” act aims to improve equity and reduce discrimination
2.8. Person-centred care
In July 2025, the Government of Slovenia adopted the National Strategy for Health Literacy 2025–2035 and the action plan related to the strategy for the first two years of its implementation. Health literacy contributes to equity, efficiency and sustainability of the health system. Studies carried out in Slovenia showed the need for improvement in health literacy in the population. For example, in 2020 a major survey on health literacy showed limited health literacy in 48% of respondents in Slovenia (Vrdelja, 2022).
The strategy pursues nine objectives ultimately aimed at improving health literacy: empowering citizens in health decision-making, strengthening the knowledge of children and adolescents, better communication in health institutions, additional training for health professionals, promoting digital health literacy, assisting vulnerable groups and patients with chronic diseases, lifelong health learning, greater role of civil society and communities, and integrating health literacy into public policies and international cooperation. To achieve each objective between two and five tasks were identified. These will be further developed in biannual action plans, the first of which has already been published with the strategy. An example of concrete action is “Preparation of national guidelines for clear, structured and adapted communication of health content in institutions (written, oral, digital communication)”.
Authors
References
Ministry of Health of the Republic of Slovenia, 2025. Sprejeta Nacionalna strategija za izboljšanje zdravstvene pismenosti [National Strategy for Improving Health Literacy Adopted] Available at https://www.gov.si/novice/2025-07-17-sprejeta-nacionalna-strategija-za-izboljsanje-zdravstvene-pismenosti
Vrdelja, M., Vrbovšek, S., Berzelak, N. (2022). Zdravstvena pismenost odraslih v Sloveniji: rezultati Nacionalne raziskave zdravstvene pismenosti v Sloveniji (HLS-SI19). [Health literacy of adults in Slovenia: results of the National Health Literacy Survey in Slovenia (HLS-SI19)] Ljubljana: Nacionalni inštitut za javno zdravje. Available at https://nijz.si/wp-content/uploads/2022/12/porocilo_hls-si19_si.pdf
2.8.1. Patient information
Several sources of information are available for patients to guide them through the health care system (Table2.3). The websites of the MoH, ZZZS, NIJZ and health care providers are the main sources of information. ZZZS provides information on benefits, how citizens and residents can settle their compulsory health insurance status and about public provider organizations. It also offers periodic updates on the availability of individual family medicine specialists[3] and other primary care providers in the public network. The NIJZ publishes electronically monitored waiting times (updated monthly) by provider for a limited number of services. These data are self-reported by the providers, and to counteract reporter bias, the MoH is currently planning to introduce measures to ensure reporting accuracy and timeliness by the providers. Most of this information can also be retrieved through the National Contact Point, which was established according to the requirements of EU Directive 2011/24/EU on patient rights in cross-border health care (see section 2.8.4).
Table2.3
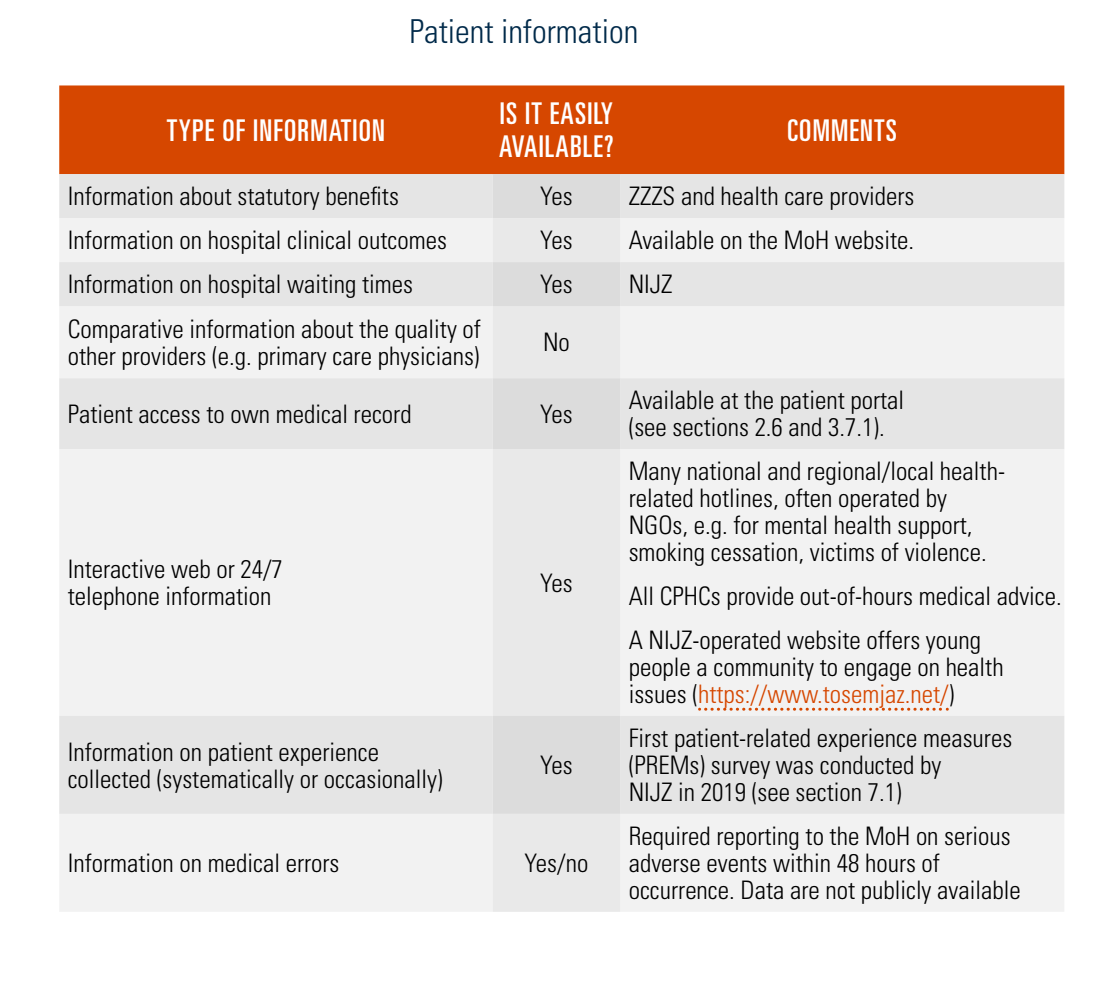
For the two autochthonous ethnic minorities in Slovenia (Italians in the south-west and Hungarians in the north-east), some local health care institutions are obliged to offer information in Slovene and an autochthonous language. Information brochures and health promotion materials may also be provided in English, Albanian and certain other languages. Further, according to European legislation, patient information leaflets must be enclosed with each medicinal product placed on the market.
- 3. In Slovenia, since 2000, all physicians working in family medicine practices are required to have four-year specialization (residency) in family medicine. GPs with only medical faculty diploma are no longer allowed to work with patients. ↰
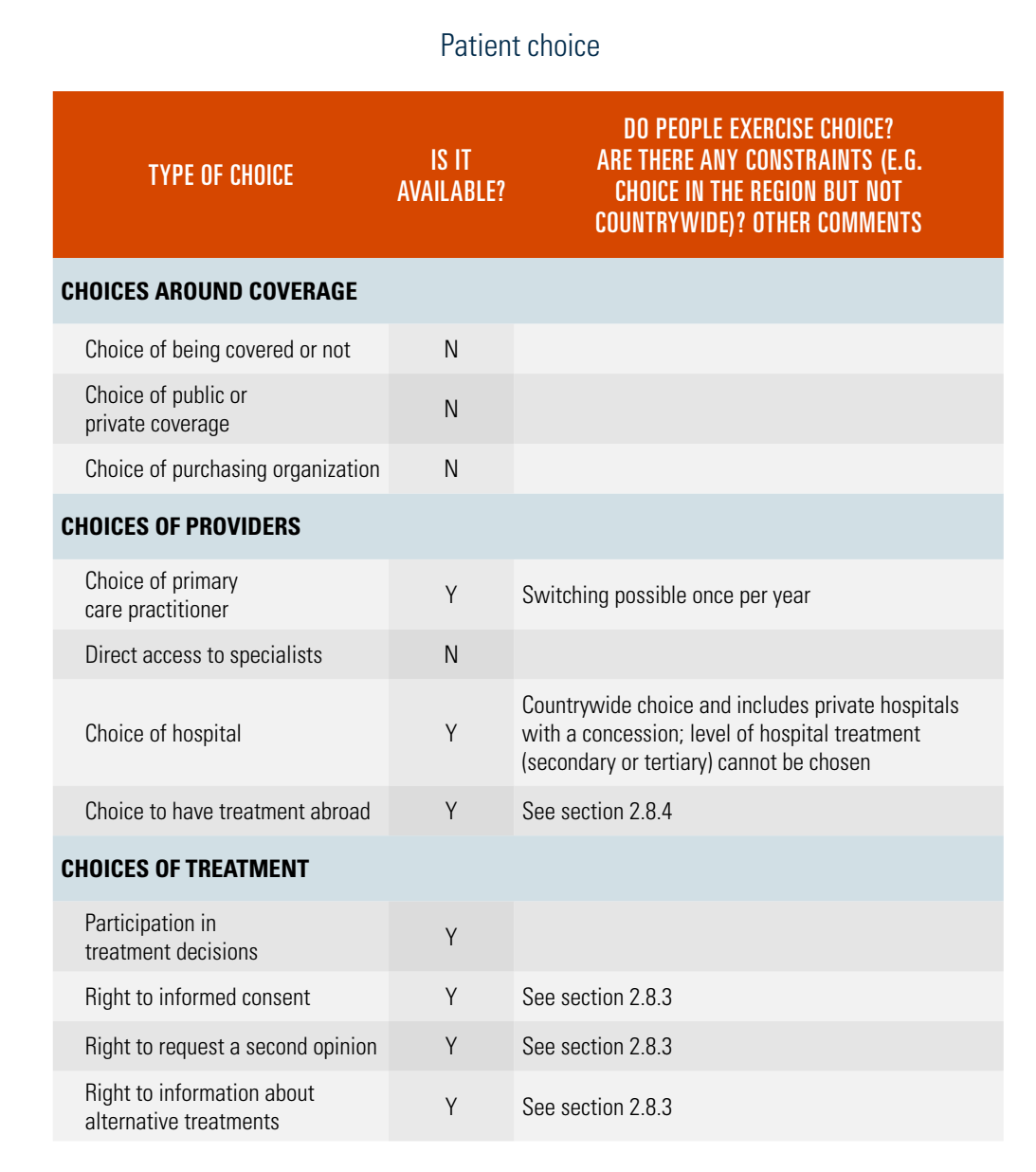
2.8.2. Patient choice
Statutory coverage via the single national insurance fund is obligatory and opting out is not permitted. There is no choice of the statutory benefits package. Patients can choose their personal primary care provider (family medicine specialists, paediatricians, gynaecologists, dentists), who act as gatekeepers, providing access to secondary and tertiary care through referrals (see section 5.3). Patients may choose their specialist providers with a referral without administrative or geographical constraint.
Patients have free choice of complementary insurance (covering co-insurance in the form of co-payments), which is offered by three insurance companies (see sections 2.2 and 3.5). These companies, along with several others, also offer supplementary insurance packages (e.g. for some ambulatory specialist services, specialist visits outside the public network and to circumvent waiting times), though the Slovene supplementary insurance market is small (Table2.4).
Table2.4
2.8.3. Patient rights
Patient rights and responsibilities are regulated by the Patients’ Rights Act (2008, amended in 2017 and 2020). In line with the WHO Declaration on the Promotion of Patients’ Rights in Europe (WHO, 1994), which distinguishes between social and individual rights, the Act is mainly concerned with individual rights (Table2.5).[4]
Table2.5
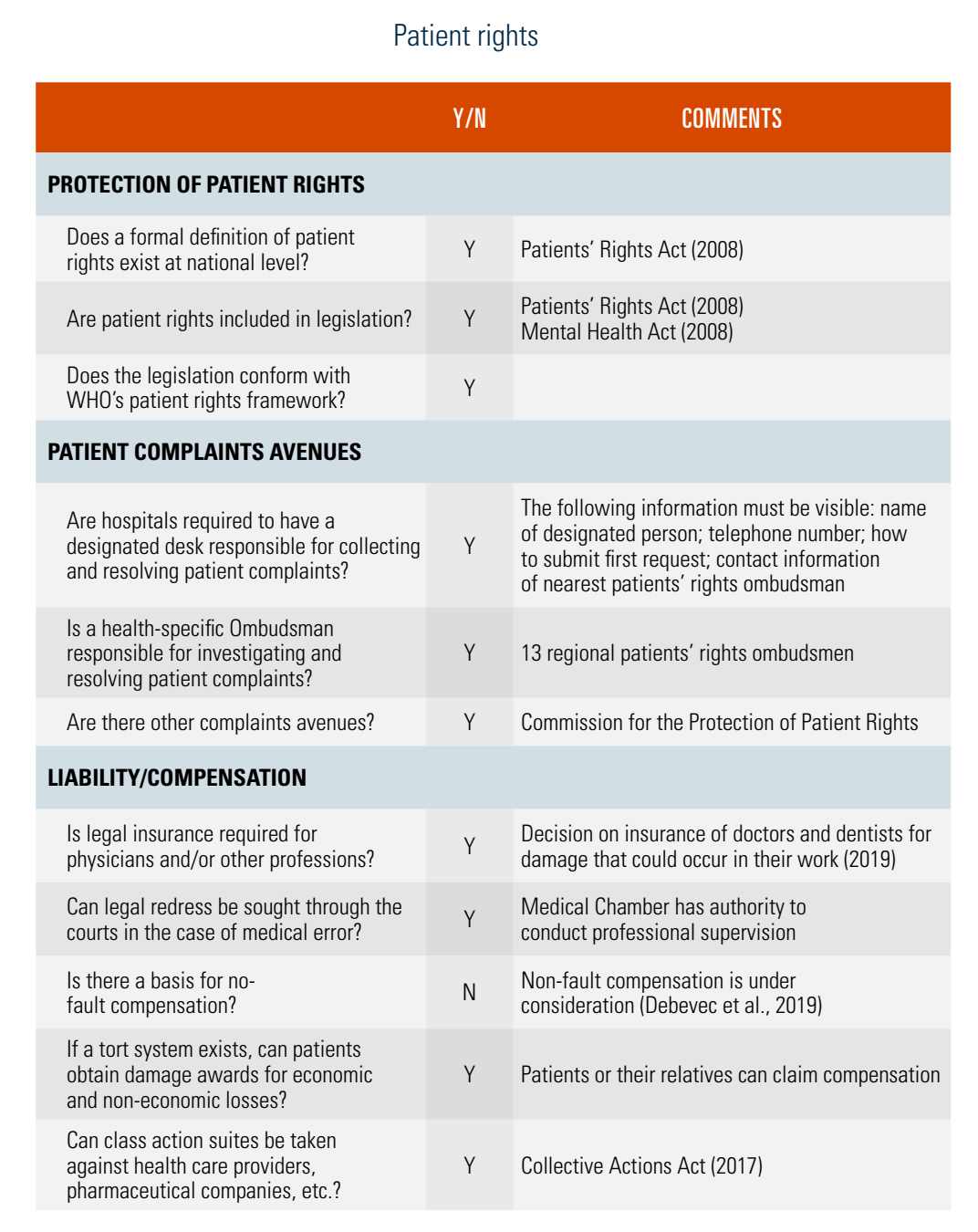
The Act (article 5) lists 14 patient rights and divides them according to level of engagement in the health system, such as rights expected as a user of health services, as a patient of providers and procedural rights, including the right to have decisions reviewed and those related to the violation of other rights.
It also describes patient duties related to these rights. In practice, realization of these rights is conditioned by the right to health care services and by evidence-based medical doctrine and standards (e.g. physicians have the right to refuse treatment if it is not medically indicated or is subject to concerns related to medical ethics).
Furthermore, the Act introduces 13 patients’ rights ombudsmen, who are nominated by the MoH and responsible for regions, and the Commission for the Protection of Patient Rights, which provides support to patients and report annually to the government.
- 4. The social rights of patients, which mainly relate to the basket of services covered by compulsory and complementary health insurance, are set out in the Health Care and Health Insurance Act 2006 (and its subsequent amendments; see also section 3.3.1). ↰
In November 2024 Slovenia adopted the “Law on the right of persons who have survived cancer and certain other diseases to equal access to insurance and credit products”. The main provision of the law relates to the rights of persons who have had cancer or been infected with hepatitis C or HIV to not disclose their history with the mentioned conditions and the obligation for insurance or crediting institutions to not consider these aspects of the medical history when evaluating a person’s request for an insurance or loan.
In principle, the right to be forgotten applies seven years after the end of active treatment of cancer, three months after the end of successful treatment of hepatitis C, and one year after the beginning of active treatment for HIV. The law also foresees particular circumstances where these timelines might be shortened.
Authors
References
2.8.4. Patients and cross-border health care
According to the EU Directive 2011/24/EU on patients in cross-border health care, EU citizens have the right to access health care in any EU country and be reimbursed for care abroad by their home country,[5] with differences between unplanned emergency treatment and planned treatment.
Insured people from one EU/EEA country are entitled to all public, emergency medical services in another, under the same conditions and for the same costs as the insured of the providing country. Slovenia has additional bilateral agreements for cross-border emergency health care with Australia, Bosnia and Herzegovina, Montenegro, North Macedonia, Serbia and Switzerland. Emergency medical services received in other countries are reimbursed (by ZZZS) only up to the average price of performed services in Slovenia, and not exceeding actual cost of services. People insured in an EU/EEA country may seek planned treatment abroad in three cases, each with its own legal basis, reimbursement regimes and approval procedure: 1) all treatment options in Slovenia have been exhausted; 2) waiting times exceed the maximum permissible waiting times or a reasonable period of time; or 3) the insured patient decides to receive treatment abroad on the basis of a previously issued referral and prior ZZZS approval. Primary health services cannot currently be sought outside of Slovenia.
Cross-border care represents a loss in revenue for Slovenia. Overall, 85 416 foreign citizens, mostly from Austria, Croatia, Germany and Italy, sought medical care in Slovenia in 2020, amounting to €25 411 583, while 86 761 people insured in Slovenia received health services abroad, totalling €35 980 774, mostly in Bosnia and Herzegovina (35%), Croatia (23%) and Germany (13%). The data suggest that care is sought abroad primarily because certain hospital-related procedures are not being delivered in Slovenia and because of long waiting times (see section 7.2). When looking at specific grounds, 469 applications due to exhausted treatment options were approved in 2020, including for paediatric heart surgery and biomedically assisted fertilization. Twenty-two were approved, mostly for DaTscan (for diagnosis of Parkinson’s disease) in Croatia, because of exceeded waiting times, and 1180 applications were received for reimbursement of specialist care or medical products based on a previously issued referral or approval from ZZZS, mostly for dental services, electromyography tests and cardiovascular surgery.
- 5. EU Directive 2011/24/EU on patients in cross-border health care sets out the conditions under which a patient may travel to another EU country to receive medical care and reimbursement. It covers health care costs, as well as the prescription and delivery of medications and medical devices. ↰