-
30 September 2022 | Policy Analysis
Implementation of methodological centres
7.4. Financial protection
The degree of financial protection provided by a health system is determined by the extent to which people are protected from the financial consequences of illness. High OOP payments in Latvia limit financial protection for individuals and households. The proportion of health expenditure paid out of pocket was around 35% in the mid-2000s but has risen to 41.8% in 2017, a level much higher than in other EU countries. Unsurprisingly, 72.8% of low-income Latvian households (and 61.9% of the whole Latvian population) reported using health care services but reported having some, moderate or great difficulty in affording them in 2016 (Eurostat, 2019).
In Latvia, the population – and especially the poorest income quintile – is at risk of catastrophic health expenditure and impoverishment due to high OOP expenditure (catastrophic expenditure is defined as household OOP spending exceeding 40% of total household spending net of subsistence needs, i.e. food, housing and utilities). A substantial share of Latvian households reports catastrophic health expenditure, far above EU18 average and among the highest in the countries with data available (Fig7.3). Further, almost half of all households incurring catastrophic health expenditure are in the poorest quintile, with more than one in four low-income households facing catastrophic OOP spending. In particular, pensioners are most exposed to catastrophic OOP payments due to ill health (Taube et al., 2015).
Fig7.3
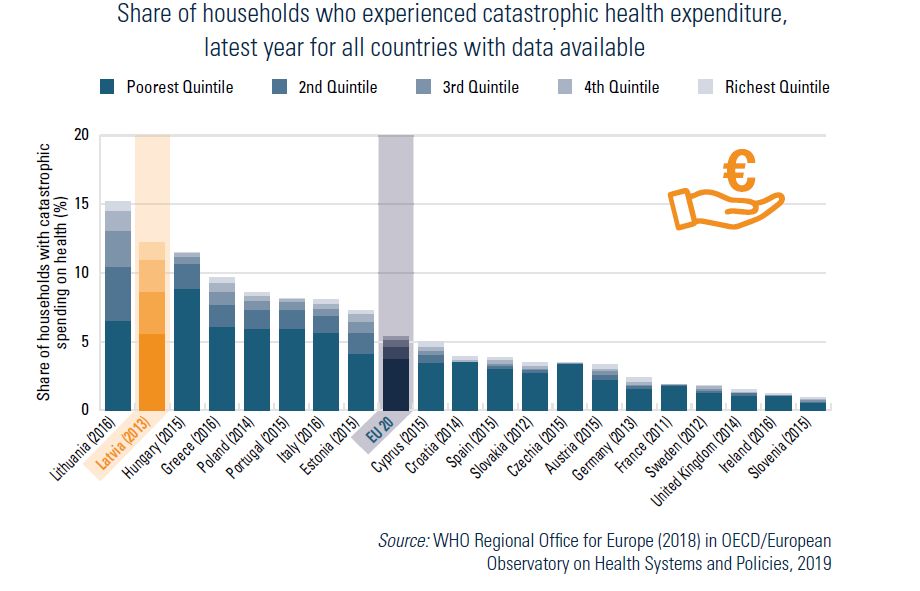
The largest share of OOP payments is absorbed by pharmaceuticals and medical devices. Better access to medicines and improving affordability are policy priorities.
There are a number of mechanisms in place to protect people from catastrophic spending or underutilization of required services. Very poor households have been exempted from all user charges since 2009. Other exempt groups include children under the age of 18 years, pregnant women, severely disabled people, etc. Yet, although there is an annual cap on user charges for all the population, this does not apply to outpatient medicines.
Addressing the high share of OOP expenditure is a major priority towards ensuring financial protection for individuals and households. Previous research indicated that financial hardship is more likely to occur when public spending on health is low in relation to GDP and OOP payments account for a considerable share of total health expenditure (Xu et al., 2007; WHO, 2010; 2018b). Recent reforms introduced additional sources of funding (social contributions) in order to diversify the funding stream. Nevertheless, these reforms need to tackle OOP payments first (see Chapter 6) if the inequality in the system is to be addressed.
To create unified management of health care services and a unified approach to the provision of health care services, as well as to ensure uniform quality monitoring, a new proposal is to create methodological management centres in separate medical areas. Currently, there are no established clinical methodological management institutions for medical branches in Latvia, which would deal with quality control and principles of prevention, diagnosis, treatment and follow-up.
The methodological management centre will be a medical institution or its structural unit, which will develop uniform principles of prevention, diagnosis and treatment in the relevant field of health care (clinical pathways and clinical guidelines) and ensure systematic monitoring of the quality of the treatment process, performing methodological management of medical institutions in the relevant field of health care. These centres will not only provide the centralization of highly specialized services and training for health care specialists, but will share their knowledge and experience of the best standards of care.
According to the proposal for the improvement of healthcare services in the field of oncology for 2022–2024, the initial plan is to create a methodical management institution in oncology, followed by two further priorities: cardiology and psychiatry. In total, the plans are to create nine centres.
However, this will need to be supported by changes in regulation.